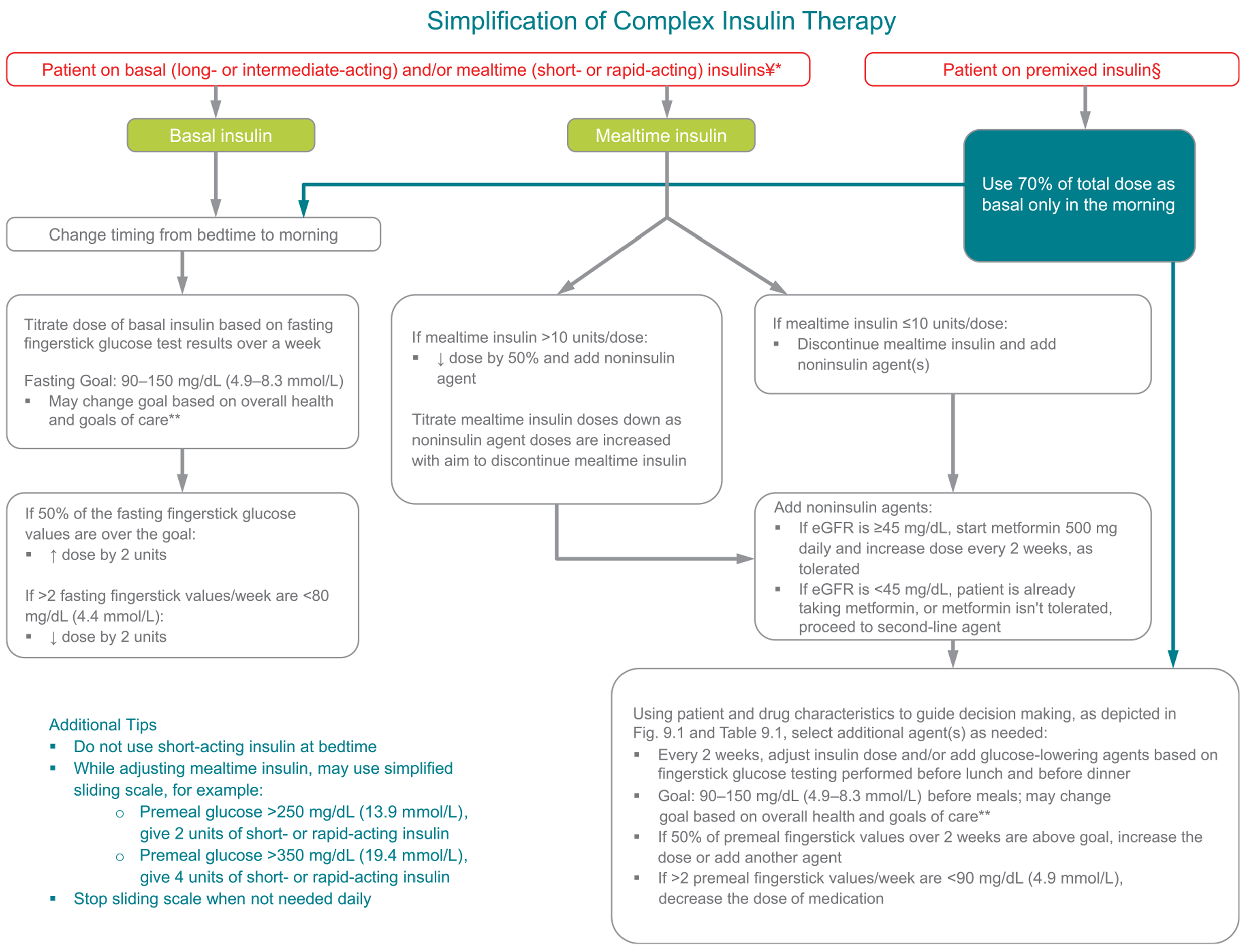
Fig. 12.1 —Algorithm to simplify insulin regimen for older patients with type 2 diabetes. eGFR, estimated glomerular filtration rate.
*Basal insulins: glargine U-100 and U-300, detemir, degludec, and human NPH.
**See Table 12.1. ¥Mealtime insulins: short-acting (regular human insulin) or rapidacting (lispro, aspart, and glulisine).
§Premixed insulins: 70/30, 75/25, and 50/50 products. Adapted with permission from Munshi and colleagues (39,55,56).
Special care is required in prescribing and monitoring pharmacologic therapies in older adults (33). See Fig. 9.1 for general recommendations regarding antihyperglycemia treatment for adults with type 2 diabetes and Table 9.1 for patient- and drug-specific factors to consider when selecting antihyperglycemia agents. Cost may be an important consideration, especially as older adults tend to be on many medications. See Tables 9.2 and 9.3 for median monthly cost of noninsulin glucose-lowering agents and insulin in the U.S., respectively. It is important to match complexity of the treatment regimen to the self-management ability of an older patient. Many older adults with diabetes struggle to maintain the frequent blood glucose testing and insulin injection regimens they previously followed, perhaps for many decades, as they develop medical conditions that may impair their ability to follow their regimen safely. Individualized glycemic goals should be established (Fig. 6.1) and periodically adjusted based on coexisting chronic illnesses, cognitive function, and functional status (2). Tight glycemic control in older adults with multiple medical conditions is considered overtreatment and is associated with an increased risk of hypoglycemia; unfortunately, overtreatment is common in clinical practice (34-38). Deintensification of regimens in patients taking noninsulin glucose-lowering medications can be achieved by either lowering the dose or discontinuing some medications, so long as the individualized A1C target is maintained. When patients are found to have an insulin regimen with complexity beyond their self-management abilities, lowering the dose of insulin may not be adequate. Simplification of the insulin regimen to match an individual’s self-management abilities in these situations has been shown to reduce hypoglycemia and disease-related distress without worsening glycemic control (39-41). Figure 12.1 depicts an algorithm that can be used to simplify the insulin regimen (39). Table 12.2 provides examples of and rationale for situations where deintensification and/or insulin regimen simplification may be appropriate in older adults.
Metformin
Metformin is the first-line agent for older adults with type 2 diabetes. Recent studies have indicated that it may be used safely in patients with estimated glomerular filtration rate ≥30 mL/min/1.73 m2 (42). However, it is contraindicated in patients with advanced renal insufficiency and should be used with caution in patients with impaired hepatic function or congestive heart failure due to the increased risk of lactic acidosis. Metformin may be temporarily discontinued before procedures, during hospitalizations, and when acute illness may compromise renal or liver function.
Thiazolidinediones
Thiazolidinediones, if used at all, should be used very cautiously in those with, or at risk for, congestive heart failure and those at risk for falls or fractures.
Insulin Secretagogues
Sulfonylureas and other insulin secretagogues are associated with hypoglycemia and should be used with caution. If used, shorter-duration sulfonylureas, such as glipizide, are preferred. Glyburide is a longer-duration sulfonylurea and contraindicated in older adults (43).
Incretin-Based Therapies
Oral dipeptidyl peptidase 4 (DPP-4) inhibitors have few side effects and minimal hypoglycemia, but their costs may be a barrier to some older patients. DPP-4 inhibitors do not increase major adverse cardiovascular outcomes (44).
Glucagon-like peptide 1 (GLP-1) receptor agonists are injectable agents, which require visual, motor, and cognitive skills for appropriate administration. They may be associated with nausea, vomiting, and diarrhea. Also, weight loss with GLP-1 receptor agonists may not be desirable in some older patients, particularly those with cachexia. In patients with established atherosclerotic cardiovascular disease, GLP-1 receptor agonists have shown cardiovascular benefits (44).
Table 12.2—Considerations for treatment regimen simplification and deintensification/deprescribing in older adults with diabetes (39,55)

Treatment regimen simplification refers to changing strategy to decrease the complexity of a medication regimen, e.g., fewer administration times, fewer fingerstick readings, decreasing the need for calculations (such as sliding scale insulin calculations or insulin-carbohydrate ratio calculations). Deintensification/deprescribing refers to decreasing the dose or frequency of administration of a treatment or discontinuing a treatment altogether. ADL, activities of daily living.
†Consider adjustment of A1C goal if the patient has a condition that may interfere with erythrocyte life span/turnover.
Sodium-Glucose Cotransporter 2 Inhibitors
Sodium-glucose cotransporter 2 inhibitors are administered orally, which may be convenient for older adults with diabetes; however, long-term experience in this population is limited despite the initial efficacy and safety data reported with these agents. In patients with established atherosclerotic cardiovascular disease, these agents have shown cardiovascular benefits (44).
Insulin Therapy
The use of insulin therapy requires that patients or their caregivers have good visual and motor skills and cognitive ability. Insulin therapy relies on the ability of the older patient to administer insulin on their own or with the assistance of a caregiver. Insulin doses should be titrated to meet individualized glycemic targets and to avoid hypoglycemia. Once-daily basal insulin injection therapy is associated with minimal side effects and may be a reasonable option in many older patients. Multiple daily injections of insulin may be too complex for the older patient with advanced diabetes complications, life-limiting coexisting chronic illnesses, or limited functional status. Figure 12.1 provides a potential approach to insulin regimen simplification.
Other Factors to Consider
The needs of older adults with diabetes and their caregivers should be evaluated to construct a tailored care plan. Impaired social functioning may reduce their quality of life and increase the risk of functional dependency (45). The patient’s living situation must be considered as it may affect diabetes management and support needs. Social and instrumental support networks (e.g., adult children, caretakers) that provide instrumental or emotional support for older adults with diabetes should be included in diabetes management discussions and shared decision making.
Older adults in assisted living facilities may not have support to administer their own medications, whereas those living in a nursing home (community living centers) may rely completely on the care plan and nursing support. Those receiving palliative care (with or without hospice) may require an approach that emphasizes comfort and symptom management, while de-emphasizing strict metabolic and blood pressure control.