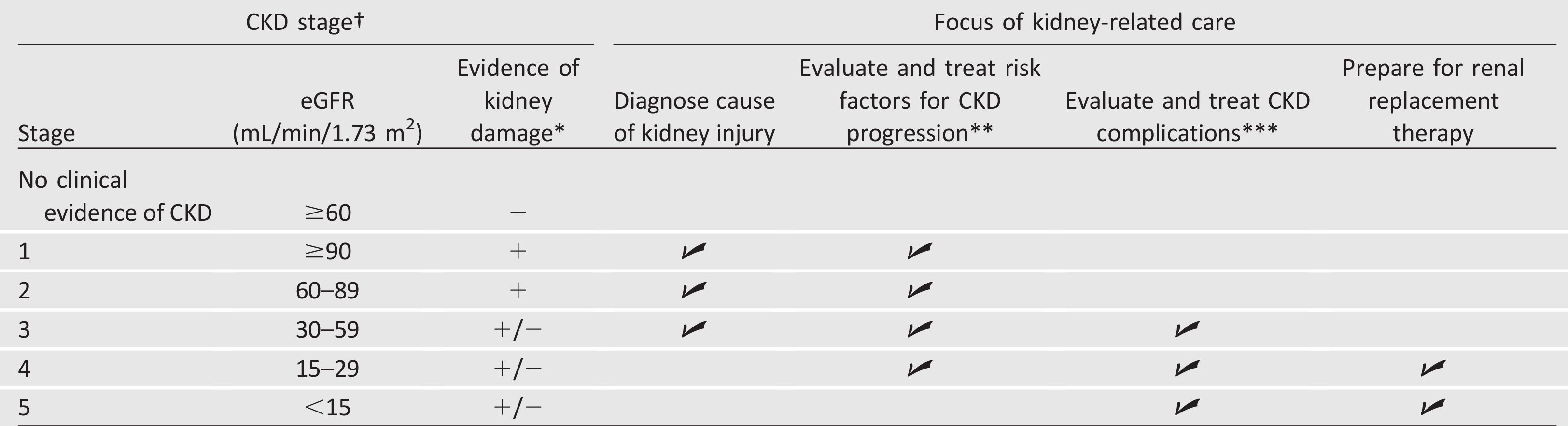
CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate. †CKD stages 1 and 2 are defined by evidence of kidney damage (+), while CKD stages 3–5 are defined by reduced eGFR with or without evidence of kidney damage (+/-). At any stage of CKD, the degree of albuminuria, observed history of eGFR loss, and cause of kidney damage (including possible causes other than diabetes) may also be used to characterize CKD, gauge prognosis, and guide treatment decisions.
*Kidney damage is most often manifest as albuminuria (UACR ≥30 mg/g Cr) but can also include glomerular hematuria, other abnormalities of the urinary sediment, radiographic abnormalities, and other presentations.
**Risk factors for CKD progression include elevated blood pressure, hyperglycemia, and albuminuria.
***See Table 11.2.
Table 11.2—Selected complications of CKD
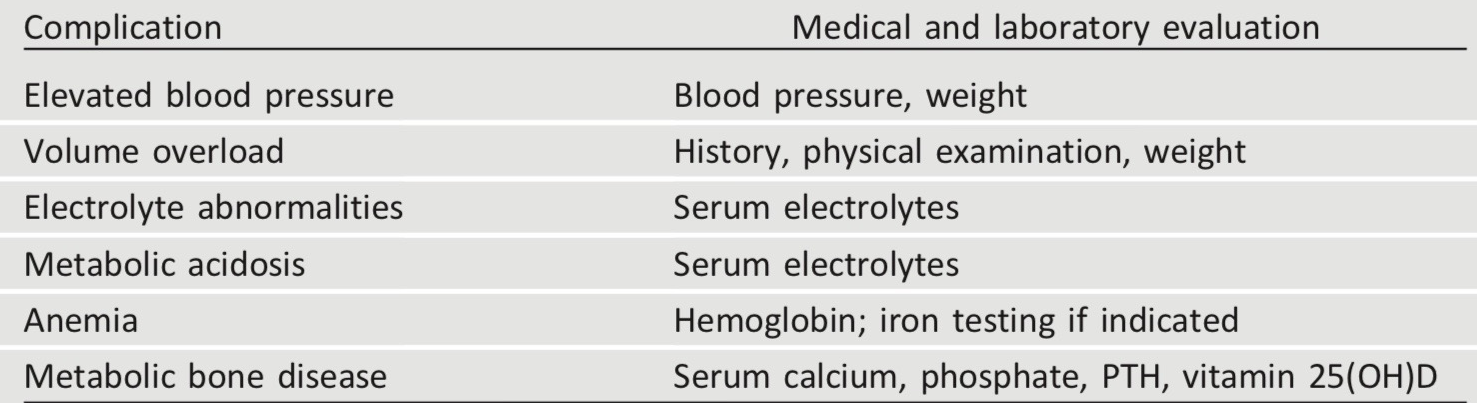
Complications of chronic kidney disease (CKD) generally become prevalent when estimated glomerular filtration rate falls below 60 mL/min/1.73 m2 (stage 3 CKD or greater) and become more common and severe as CKD progresses. Evaluation of elevated blood pressure and volume overload should occur at every clinical contact possible; laboratory evaluations are generally indicated every 6–12 months for stage 3 CKD, every 3–5 months for stage 4 CKD, and every 1–3 months for stage 5 CKD, or as indicated to evaluate symptoms or changes in therapy. PTH, parathyroid hormone; 25(OH)D, 25-hydroxyvitamin D.