6.5.0.0 Referral to a Mental Health Specialist
Indications for referral to a mental health specialist familiar with diabetes management may include positive screening for overall stress related to work-life balance, DD, diabetes management difficulties, depression, anxiety, disordered eating, and cognitive dysfunction (see Table 5.2 for a complete list). It is preferable to incorporate psychosocial assessment and treatment into routine care rather than waiting for a specific problem or deterioration in metabolic or psychological status to occur (26,193). Providers should identify behavioral and mental health providers, ideally those who are knowledgeable about diabetes treatment and the psychosocial aspects of diabetes, to whom they can refer patients. The ADA provides a list of mental health providers who have received additional education in diabetes at the ADA Mental Health Provider Directory (professional. diabetes.org/ada-mental-health-provider-directory). Ideally, psychosocial care providers should be embedded in diabetes care settings. Although the clinician may not feel qualified to treat psychological problems (200), optimizing the patient-provider relationship as a foundation may increase the likelihood of the patient accepting referral for other services. Collaborative care interventions and a team approach have demonstrated efficacy in diabetes self-management, outcomes of depression, and psychosocial functioning (17,201).
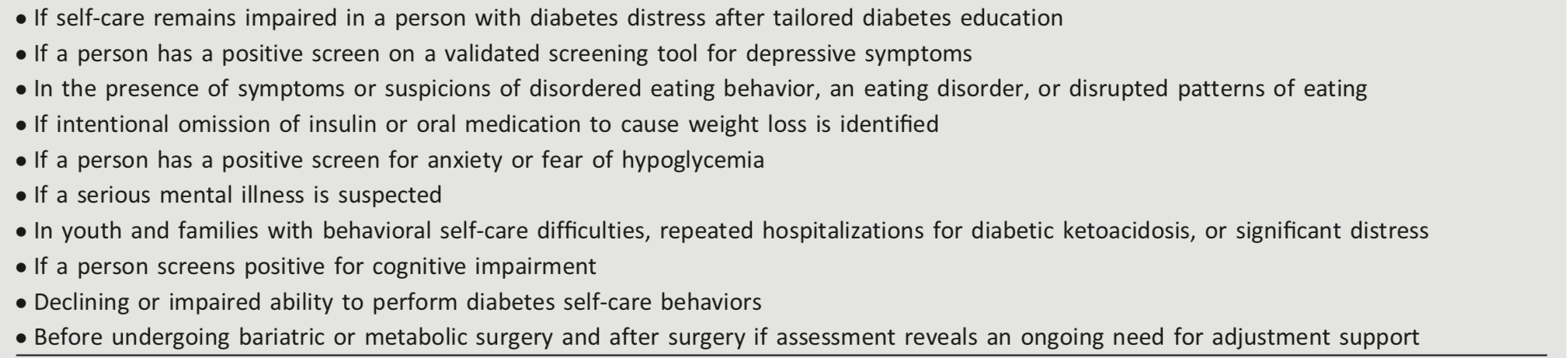
Table 5.2—Situations that warrant referral of a person with diabetes to a mental health provider for evaluation and treatment