1.0.0.0 Patient-Centered Collaborative Care
The American Diabetes Association (ADA) “Standards of Medical Care in Diabetes” includes ADA’s current clinical practice recommendations and is intended to provide the components of diabetes care, general treatment goals and guidelines, and tools to evaluate quality of care. Members of the ADA Professional Practice Committee, a multidisciplinary expert committee, are responsible for updating the Standards of Care annually, or more frequently as warranted. For a detailed description of ADA standards, statements, and reports, as well as the evidence-grading system for ADA’s clinical practice recommendations, please refer to the Standards of Care Introduction. Readers who wish to comment on the Standards of Care are invited to do so at professional.diabetes.org/SOC.
PATIENT-CENTERED COLLABORATIVE CARE
Recommendations
4.1 A patient-centered communication style that uses person-centered and strength-based language and active listening, elicits patient preferences and beliefs, and assesses literacy, numeracy, and potential barriers to care should be used to optimize patient health outcomes and health-related quality of life. B
4.2 Diabetes care should be managed by a multidisciplinary team that may draw from primary care physicians, subspecialty physicians, nurse practitioners, physician assistants, nurses, dietitians, exercise specialists, pharmacists, dentists, podiatrists, and mental health professionals. E
A successful medical evaluation depends on beneficial interactions between the patient and the care team. The Chronic Care Model (1–3) (see Section 1 “Improving Care and Promoting Health in Populations”) is a patient-centered approach to care that requires a close working relationship between the patient and clinicians involved in treatment planning. People with diabetes should receive health care from an interdisciplinary team that may include physicians, nurse practitioners, physician assistants, nurses, dietitians, exercise specialists, pharmacists, dentists, podiatrists, and mental health professionals. Individuals with diabetes must assume an active role in their care. The patient, family or support people, physicians, and health care team should together formulate the management plan, which includes lifestyle management (see Section 5 “Lifestyle Management”).
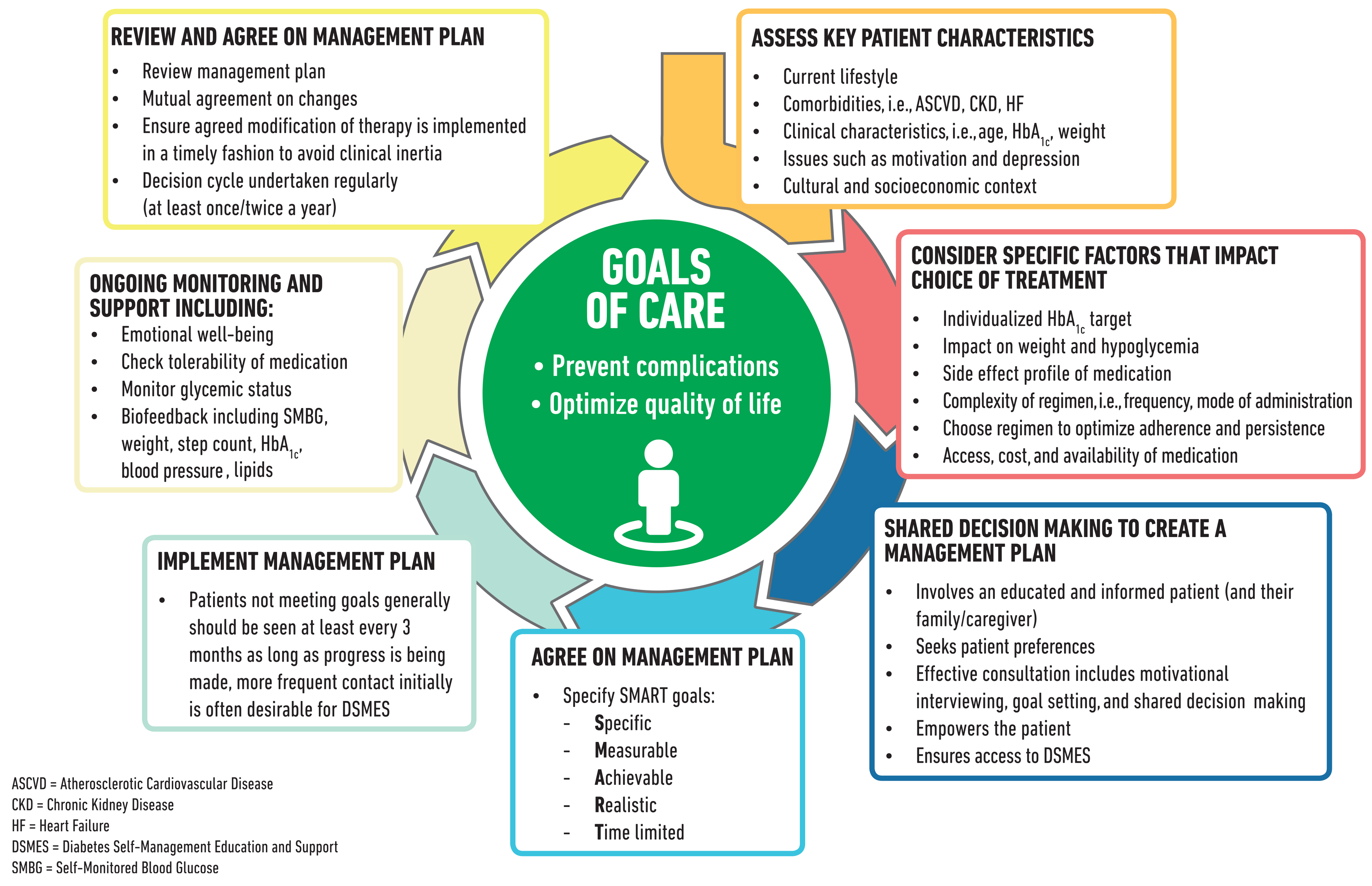
The goals of treatment for diabetes are to prevent or delay complications and maintain quality of life (Fig. 4.1). Treatment goals and plans should be created with the patients based on their individual preferences, values, and goals. The management plan should take into account the patient’s age, cognitive abilities, school/work schedule and conditions, health beliefs, support systems, eating patterns, physical activity, social situation, financial concerns, cultural factors, literacy and numeracy (mathematical literacy), diabetes complications and duration of disease, comorbidities, health priorities, other medical conditions, preferences for care, and life expectancy. Various strategies and techniques should be used to support patients’ self-management efforts, including providing education on problem-solving skills for all aspects of diabetes management.
Provider communications with patients and families should acknowledge that multiple factors impact glycemic management but also emphasize that collaboratively developed treatment plans and a healthy lifestyle can significantly improve disease outcomes and wellbeing (4–7). Thus, the goal of provider-patient communication is to establish a collaborative relationship and to assess and address self-management barriers without blaming patients for “noncompliance” or “nonadherence” when the outcomes of self-management are not optimal (8). The familiar terms “noncompliance” and “nonadherence” denote a passive, obedient role for a person with diabetes in “following doctor’s orders” that is at odds with the active role people with diabetes take in directing the day-to-day decision making, planning, monitoring, evaluation, and problem-solving involved in diabetes self-management. Using a nonjudgmental approach that normalizes periodic lapses in self-management may help minimize patients’ resistance to reporting problems with self-management. Empathizing and using active listening techniques, such as open-ended questions, reflective statements, and summarizing what the patient said, can help facilitate communication. Patients’ perceptions about their own ability, or self-efficacy, to self-manage diabetes are one important psychosocial factor related to improved diabetes self-management and treatment outcomes in diabetes (9–13) and should be a target of ongoing assessment, patient education, and treatment planning.
Language has a strong impact on perceptions and behavior. The use of empowering language in diabetes care and education can help to inform and motivate people, yet language that shames and judges may undermine this effort. The American Diabetes Association (ADA) and American Association of Diabetes Educators consensus report, “The Use of Language in Diabetes Care and Education,” provides the authors’ expert opinion regarding the use of language by health care professionals when speaking or writing about diabetes for people with diabetes or for professional audiences (14). Although further research is needed to address the impact of language on diabetes outcomes, the report includes five key consensus recommendations for language use:
Use language that is neutral, nonjudgmental, and based on facts, actions, or physiology/biology.
Use language that is free from stigma.
Use language that is strength based, respectful, and inclusive and that imparts hope.
Use language that fosters collaboration between patients and providers.
Use language that is person centered (e.g., “person with diabetes” is preferred over “diabetic”).
Figure 4.1—Decision cycle for patient-centered glycemic management in type 2 diabetes. Adapted from Davies et al. (119).
For interactive tool, see here
Suggested citation: American Diabetes Association. 4. Comprehensive medical evaluation and assessment of comorbidities: Standards of Medical Care in Diabetes-2019. Diabetes Care 2019;42(Suppl. 1):S34–S45
© 2018 by the American Diabetes Association. Readers may use this article as long as the work is properly cited, the use is educational and not for profit, and the work is not altered. More information is available at http://www.diabetesjournals .org/content/license.