1.0.0.0 CLASSIFICATION
The American Diabetes Association (ADA) “Standards of Medical Care in Diabetes” includes ADA’s current clinical practice recommendations and is intended to provide the components of diabetes care, general treatment goals and guidelines, and tools to evaluate quality of care. Members of the ADA Professional Practice Committee, a multidisciplinary expert committee, are responsible for updating the Standards of Care annually, or more frequently as warranted. For a detailed description of ADA standards, statements, and reports, as well as the evidence-grading system for ADA’s clinical practice recommendations, please refer to the Standards of Care Introduction. Readers who wish to comment on the Standards of Care are invited to do so at professional.diabetes.org/SOC.
CLASSIFICATION
Diabetes can be classified into the following general categories:
This section reviews most common forms of diabetes but is not comprehensive. For additional information, see the American Diabetes Association (ADA) position statement “Diagnosis and Classification of Diabetes Mellitus” (1).
Type 1 diabetes and type 2 diabetes are heterogeneous diseases in which clinical presentation and disease progression may vary considerably. Classification is important for determining therapy, but some individuals cannot be clearly classified as having type 1 or type 2 diabetes at the time of diagnosis. The traditional paradigms of type 2 diabetes occurring only in adults and type 1 diabetes only in children are no longer accurate, as both diseases occur in both age-groups. Children with type 1 diabetes typically present with the hallmark symptoms of polyuria/polydipsia, and approximately one-third present with diabetic ketoacidosis (DKA) (2). The onset of type 1 diabetes may be more variable in adults, and they may not present with the classic symptoms seen in children. Occasionally, patients with type 2 diabetes may present with DKA, particularly ethnic minorities (3). Although difficulties in distinguishing diabetes type may occur in all age-groups at onset, the true diagnosis becomes more obvious over time.
In both type 1 and type 2 diabetes, various genetic and environmental factors can result in the progressive loss of β-cell mass and/or function that manifests clinically as hyperglycemia. Once hyperglycemia occurs, patients with all forms of diabetes are at risk for developing the same chronic complications, although rates of progression may differ. The identification of individualized therapies for diabetes in the future will require better characterization of the many paths to β-cell demise or dysfunction (4).
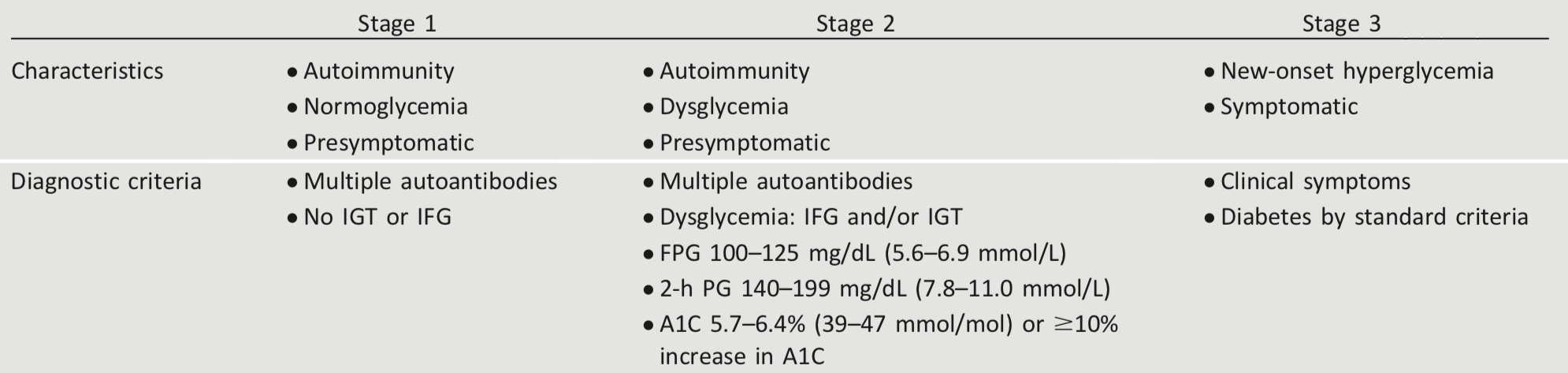
Characterization of the underlying pathophysiology is more developed in type 1 diabetes than in type 2 diabetes. It is now clear from studies of first-degree relatives of patients with type 1 diabetes that the persistent presence of two or more autoantibodies is an almost certain predictor of clinical hyperglycemia and diabetes. The rate of progression is dependent on the age at first detection of antibody, number of antibodies, antibody specificity, and antibody titer. Glucose and A1C levels rise well before the clinical onset of diabetes, making diagnosis feasible well before the onset of DKA. Three distinct stages of type 1 diabetes can be identified (Table 2.1) and serve as a framework for future research and regulatory decision making (4,5).
The paths to β-cell demise and dysfunction are less well defined in type 2 diabetes, but deficient β-cell insulin secretion, frequently in the setting of insulin resistance, appears to be the common denominator. Characterization of subtypes of this heterogeneous disorder have been developed and validated in Scandinavian and Northern European populations but have not been confirmed in other ethnic and racial groups. Type 2 diabetes is primarily associated with insulin secretory defects related to inflammation and metabolic stress among other contributors, including genetic factors. Future classification schemes for diabetes will likely focus on the pathophysiology of the underlying β-cell dysfunction and the stage of disease as indicated by glucose status (normal, impaired, or diabetes) (4).
Table 2.1 - Staging of type 1 diabetes (4,5)
Suggested citation: American Diabetes Association. 2. Classification and diagnosis of diabetes: Standards of Medical Care in Diabetesd2019. Diabetes Care 2019;42(Suppl. 1):S13–S28
© 2018 by the American Diabetes Association. Readers may use this article as long as the work is properly cited, the use is educational and not for profit, and the work is not altered. More information is available at www.diabetesjournals.org/content/license.