2.3.2.0 Randomized Controlled Trials of Intensive Versus Standard Blood Pressure Control
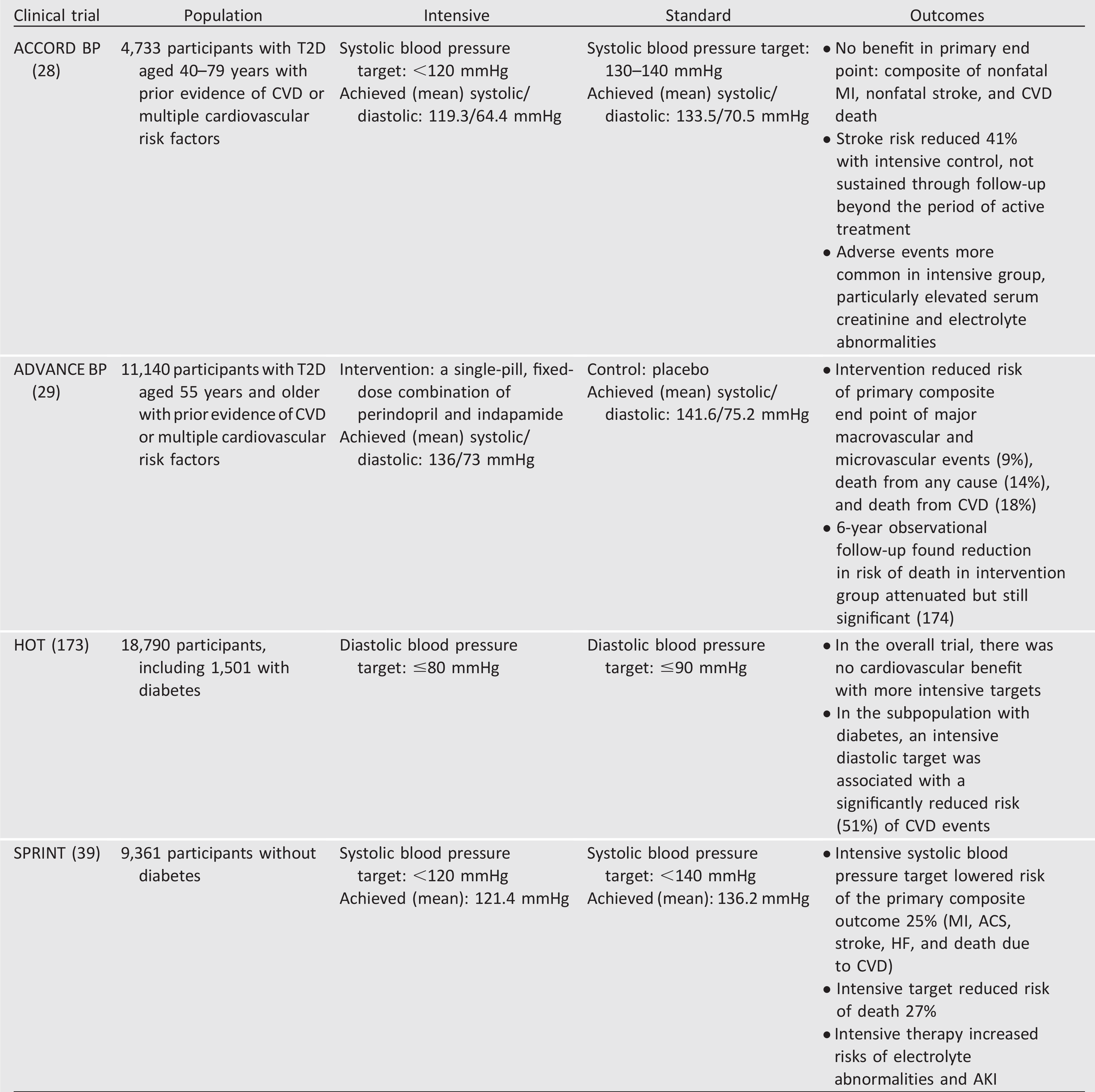
The Action to Control Cardiovascular Risk in Diabetes blood pressure (ACCORD BP) trial provides the strongest direct assessment of the benefits and risks of intensive blood pressure control among people with type 2 diabetes (28). In ACCORD BP, compared with standard blood pressure control (target systolic blood pressure <140 mmHg), intensive blood pressure control (target systolic blood pressure <120 mmHg) did not reduce total major atherosclerotic cardiovascular events but did reduce the risk of stroke, at the expense of increased adverse events (Table 10.1). The ACCORD BP results suggest that blood pressure targets more intensive than <140/90 mmHg are not likely to improve cardiovascular outcomes among most people with type 2 diabetes but may be reasonable for patients who may derive the most benefit and have been educated about added treatment burden, side effects, and costs, as discussed below.
Additional studies, such as the Systolic Blood Pressure Intervention Trial (SPRINT) and the Hypertension Optimal Treatment (HOT) trial, also examined effects of intensive versus standard control (Table 10.1), though the relevance of their results to people with diabetes is less clear. The Action in Diabetes and Vascular Disease: Preterax and Diamicron MR Controlled Evaluation–Blood Pressure (ADVANCE BP) trial did not explicitly test blood pressure targets (29); the achieved blood pressure in the intervention group was higher than that achieved in the ACCORD BP intensive arm and would be consistent with a target blood pressure of <140/90 mmHg. Notably, ACCORD BP and SPRINT measured blood pressure using automated office blood pressure measurement, which yields values that are generally lower than typical office blood pressure readings by approximately 5–10 mmHg (30), suggesting that implementing the ACCORD BP or SPRINT protocols in an outpatient clinic might require a systolic blood pressure target higher than <120 mmHg, such as <130 mmHg.
A number of post hoc analyses have attempted to explain the apparently divergent results of ACCORD BP and SPRINT. Some investigators have argued that the divergent results are not due to differences between people with and without diabetes but rather are due to differences in study design or to characteristics other than diabetes (31-33). Others have opined that the divergent results are most readily explained by the lack of benefit of intensive blood pressure control on cardiovascular mortality in ACCORD BP, which may be due to differential mechanisms underlying cardiovascular disease in type 2 diabetes, to chance, or both (34).
Table 10.1—Randomized controlled trials of intensive versus standard hypertension treatment strategies