2.0.0.0 COMPREHENSIVE MEDICAL EVALUATION
Recommendations
4.3 A complete medical evaluation should be performed at the initial visit to:
Confirm the diagnosis and classify diabetes. B
Evaluate for diabetes complications and potential comorbid conditions. B
Review previous treatment and risk factor control in patients with established diabetes. B
Begin patient engagement in the formulation of a care management plan. B
Develop a plan for continuing care. B
4.4 A follow-up visit should include most components of the initial comprehensive medical evaluation including: interval medical history, assessment of medication-taking behavior and intolerance/ side effects, physical examination, laboratory evaluation as appropriate to assess attainment of A1C and metabolic targets, and assessment of risk for complications, diabetes self-management behaviors, nutrition, psychosocial health, and the need for referrals, immunizations, or other routine health maintenance screening. B
4.5 Ongoing management should be guided by the assessment of diabetes complications and shared decision making to set therapeutic goals. B
4.6 The 10-year risk of a first atherosclerotic cardiovascular disease event should be assessed using the race- and sex-specific Pooled Cohort Equations to better stratify atherosclerotic cardiovascular disease risk. B
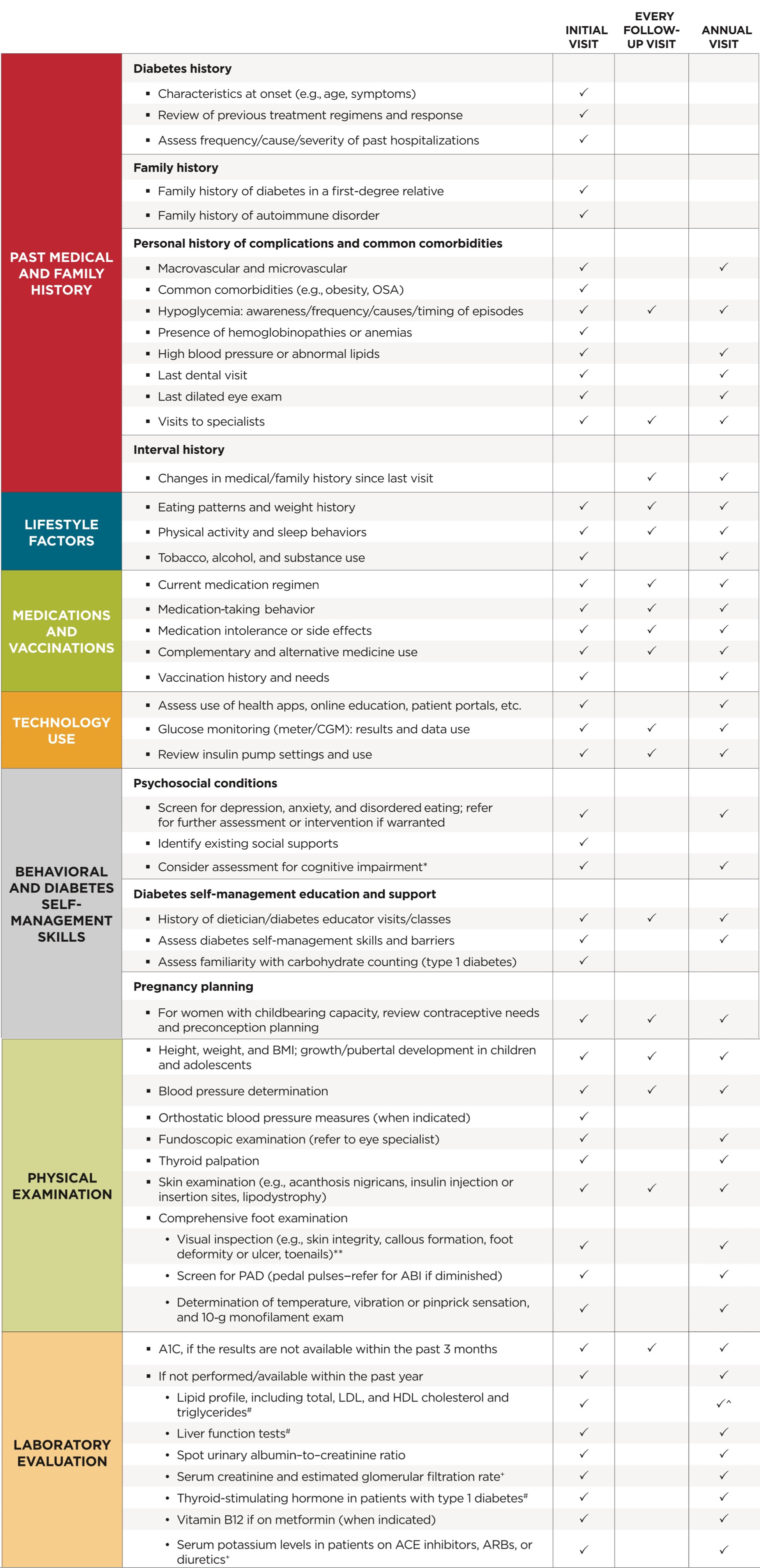
The comprehensive medical evaluation includes the initial and follow-up evaluations, assessment of complications, psychosocial assessment, management of comorbid conditions, and engagement of the patient throughout the process. While a comprehensive list is provided in Table 4.1, in clinical practice, the provider may need to prioritize the components of the medical evaluation given the available resources and time. The goal is to provide the health care team information to optimally support a patient. In addition to the medical history, physical examination, and laboratory tests, providers should assess diabetes self-management behaviors, nutrition, and psychosocial health (see Section 5 “Lifestyle Management”) and give guidance on routine immunizations. The assessment of sleep pattern and duration should be considered; a recent meta-analysis found that poor sleep quality, short sleep, and long sleep were associated with higher A1C in people with type 2 diabetes (15). Interval follow-up visits should occur at least every 3–6 months, individualized to the patient, and then annually.
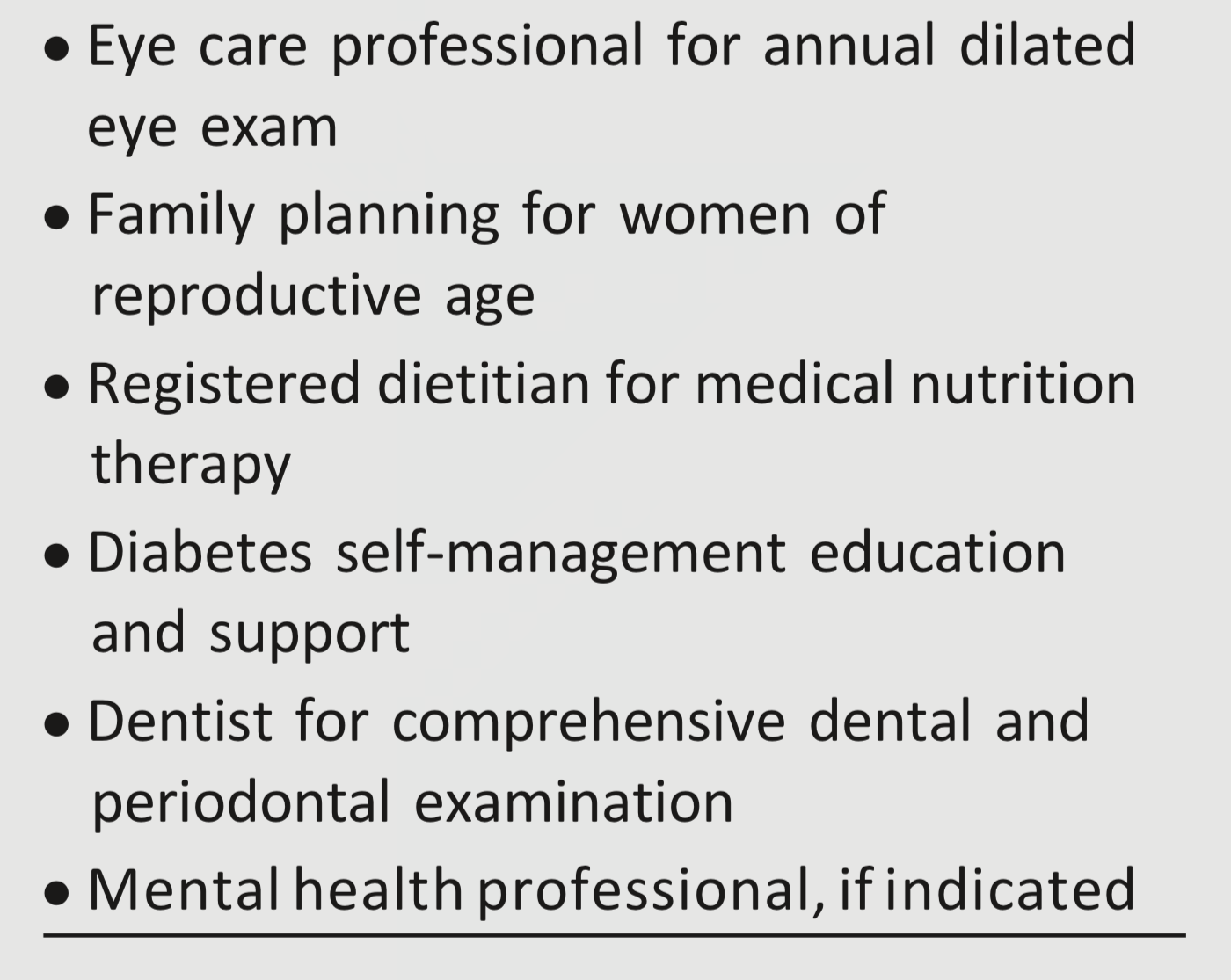
Lifestyle management and psychosocial care are the cornerstones of diabetes management. Patients should be referred for diabetes self-management education and support, medical nutrition therapy, and assessment of psychosocial/emotional health concerns if indicated. Patients should receive recommended preventive care services (e.g., immunizations, cancer screening, etc.), smoking cessation counseling, and ophthalmological, dental, and podiatric referrals.
The assessment of risk of acute and chronic diabetes complications and treatment planning are key components of initial and follow-up visits (Table 4.2). The risk of atherosclerotic cardiovascular disease and heart failure (Section 10 “Cardiovascular Disease and Risk Management”), chronic kidney disease staging (Section 11 “Microvascular Complications and Foot Care”), and risk of treatment-associated hypoglycemia (Table 4.3) should be used to individualize targets for glycemia (Section 6 “Glycemic Targets”), blood pressure, and lipids and to select specific glucose-lowering medication (Section 9 “Pharmacologic Approaches to Glycemic Treatment”), antihypertension medication, or statin treatment intensity.
Additional referrals should be arranged as necessary (Table 4.4). Clinicians should ensure that individuals with diabetes are appropriately screened for complications and comorbidities. Discussing and implementing an approach to glycemic control with the patient is a part, not the sole goal, of the patient encounter.
Table 4.1 Components of the comprehensive diabetes medical evaluation at initial, follow-up, and annual visits
ABI, ankle-brachial pressure index: ARBs, angiotensin receptor blockers; CGM, continuous glucose monitors; OSA, obstructive sleep apnea; PAD, peripheral arterial disease
'at 65 years of age or older
+may be needed more frequently in patients with known chronic kidney disease or with changes in medications that affect kidney function and serum potassium (see Table 11.2)
#may also need to be checked after initiation or dose changes of medications that affect these laboratory values (i.e., diabetes medications, blood pressure medications, cholesterol medications, or thyroid medications)
^in people without dyslipidemia and not on cholesterol lowering therapy, testing may be less frequent.
**should be performed at every visit in patients with sensory loss, previous foot ulcers, or amputations
Table 4.2—Assessment and treatment plan*
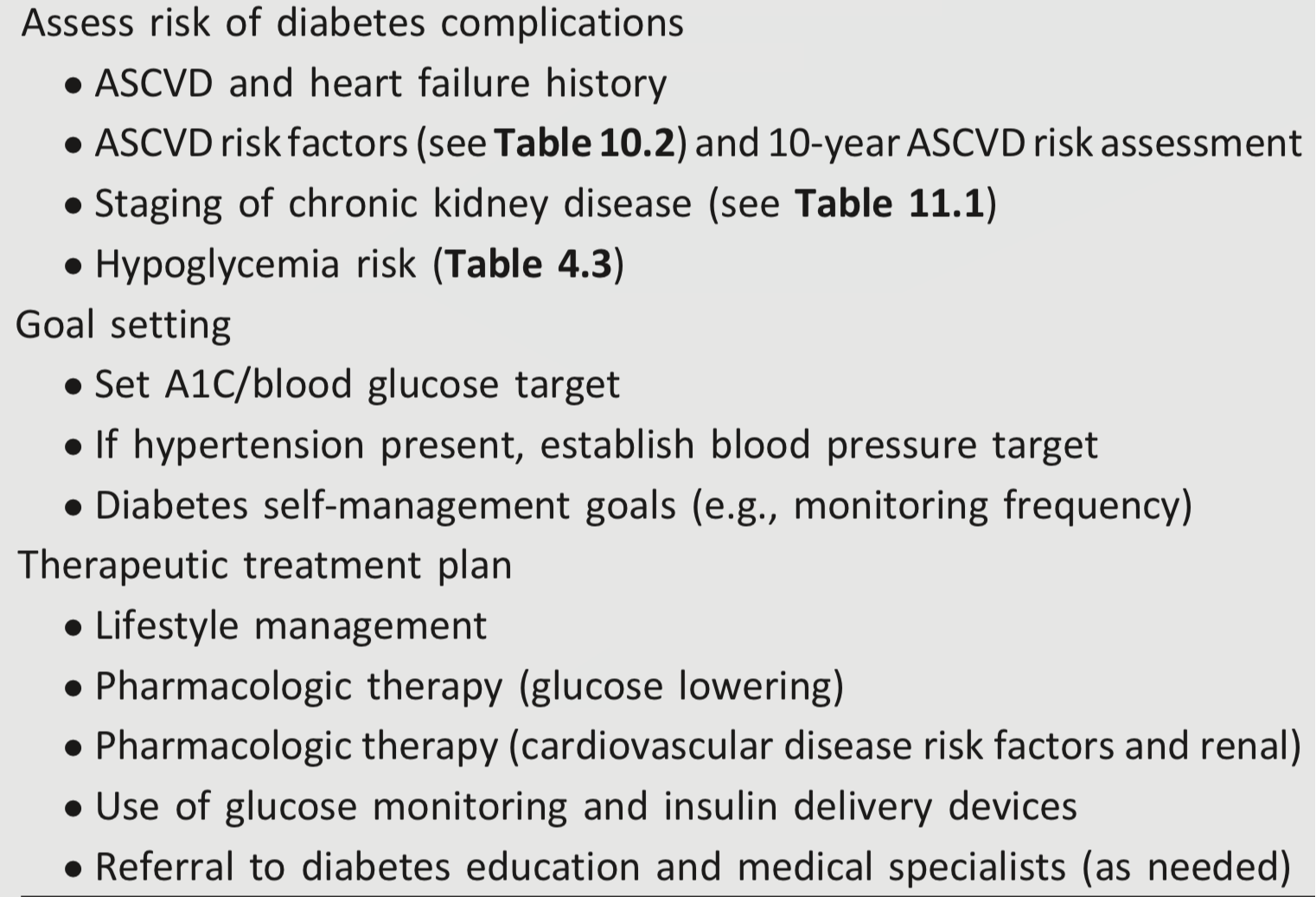
ASCVD, atherosclerotic cardiovascular disease.
*Assessment and treatment planning is an essential component of initial and all follow-up visits.
Table 4.3—Assessment of hypoglycemia risk
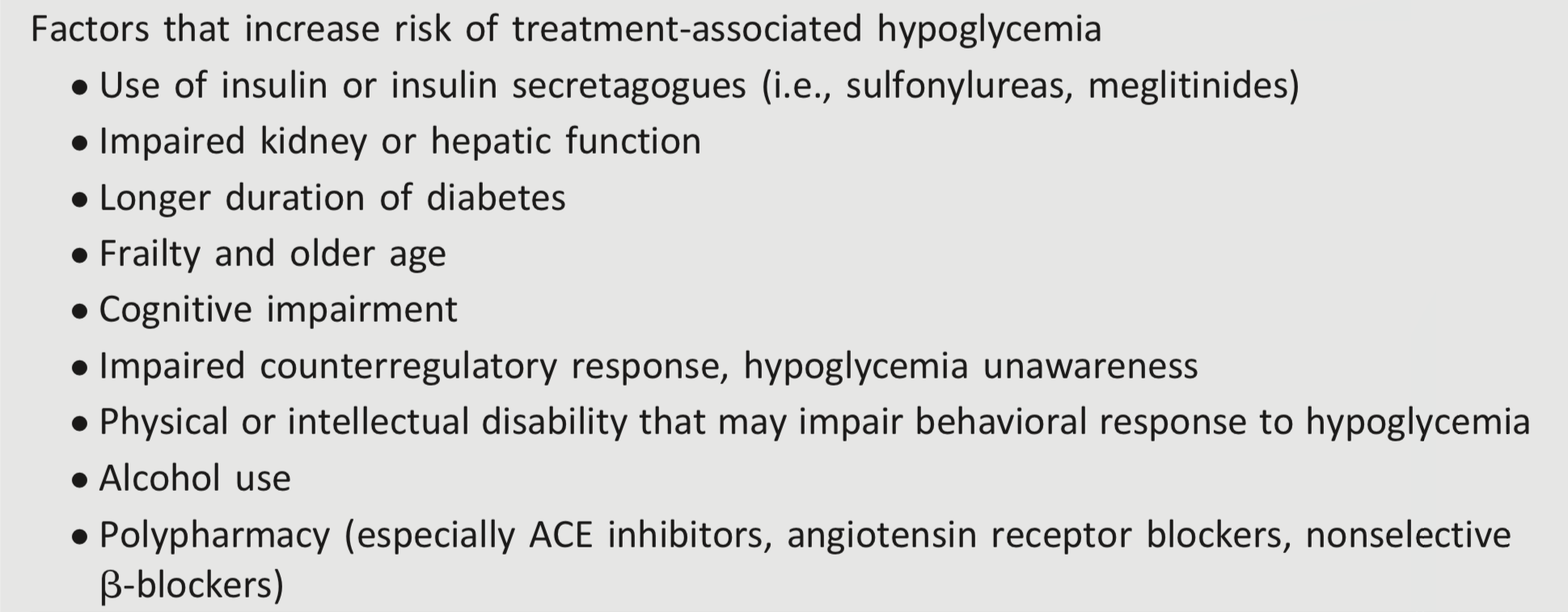
See references 114–118.
Table 4.4—Referrals for initial care management