5.3.0.0 Diagnosis
5.3.1.0 Overview
GDM carries risks for the mother, fetus, and neonate. Not all adverse outcomes are of equal clinical importance. The Hyperglycemia and Adverse Pregnancy Outcome (HAPO) study (74), a large-scale multinational cohort study completed by more than 23,000 pregnant women, demonstrated that risk of adverse maternal, fetal, and neonatal outcomes continuously increased as a function of maternal glycemia at 24–28 weeks of gestation, even within ranges previously considered normal for pregnancy. For most complications, there was no threshold for risk. These results have led to careful reconsideration of the diagnostic criteria for GDM. GDM diagnosis (Table 2.6) can be accomplished with either of two strategies:
Different diagnostic criteria will identify different degrees of maternal hyperglycemia and maternal/fetal risk, leading some experts to debate, and disagree on, optimal strategies for the diagnosis of GDM.
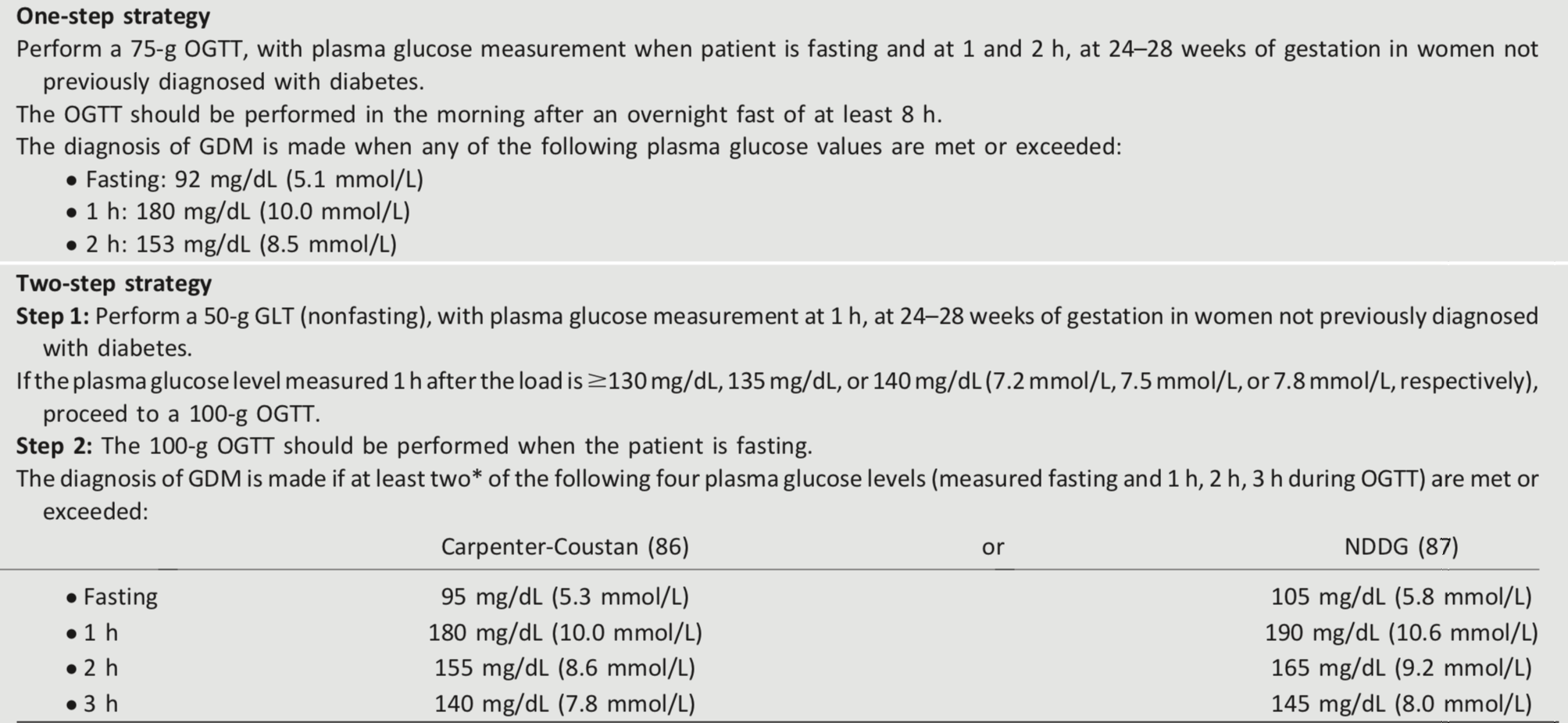
Table 2.6 - Screening for and diagnosis of GDM
NDDG, National Diabetes Data Group.
*ACOG notes that one elevated value can be used for diagnosis (82).