1.3.0.0 Grading of Scientific Evidence
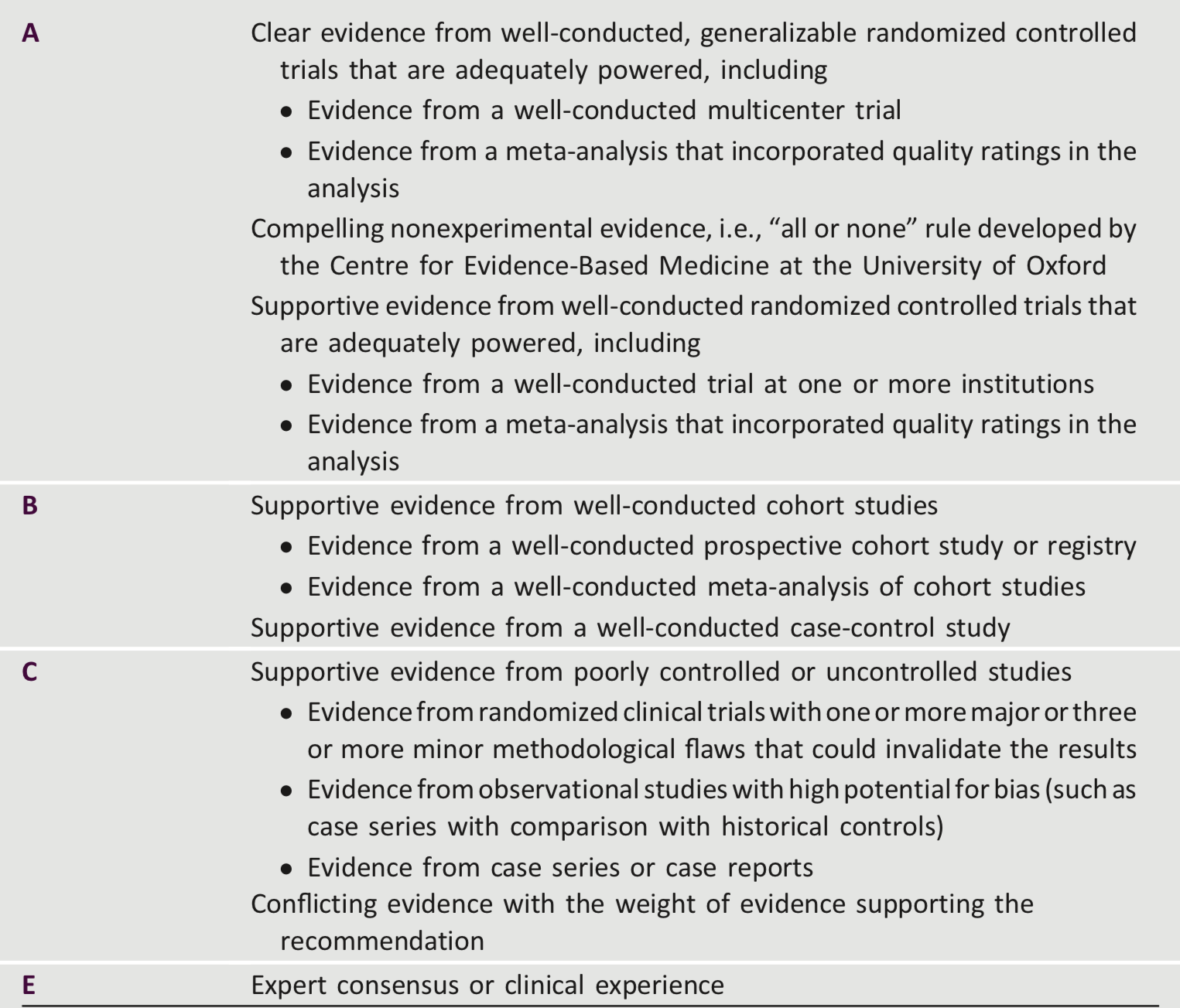
Since the ADA first began publishing practice guidelines, there has been considerable evolution in the evaluation of scientific evidence and in the development of evidence-based guidelines. In 2002, the ADA developed a classification system to grade the quality of scientific evidence supporting ADA recommendations. A 2015 analysis of the evidence cited in the Standards of Care found steady improvement in quality over the previous 10 years, with the 2014 Standards of Care for the first time having the majority of bulleted recommendations supported by A- or B-level evidence (4). A grading system (Table 1) developed by the ADA and modeled after existing methods was used to clarify and codify the evidence that forms the basis for the recommendations. ADA recommendations are assigned ratings of A, B, or C, depending on the quality of evidence. Expert opinion E is a separate category for recommendations in which there is no evidence from clinical trials, in which clinical trials may be impractical, or in which there is conflicting evidence. Recommendations with an A rating are based on large well-designed clinical trials or well-done meta-analyses. Generally, these recommendations have the best chance of improving outcomes when applied to the population to which they are appropriate. Recommendations with lower levels of evidence may be equally important but are not as well supported.
Of course, evidence is only one component of clinical decision making. Clinicians care for patients, not populations; guidelines must always be interpreted with the individual patient in mind. Individual circumstances, such as comorbid and coexisting diseases, age, education, disability, and, above all, patients’ values and preferences, must be considered and may lead to different treatment targets and strategies. Furthermore, conventional evidence hierarchies, such as the one adapted by the ADA, may miss nuances important in diabetes care. For example, although there is excellent evidence from clinical trials supporting the importance of achieving multiple risk factor control, the optimal way to achieve this result is less clear. It is difficult to assess each component of such a complex intervention.
Table 1—ADA evidence-grading system for “Standards of Medical Care in Diabetes”