2.4.2 Overview
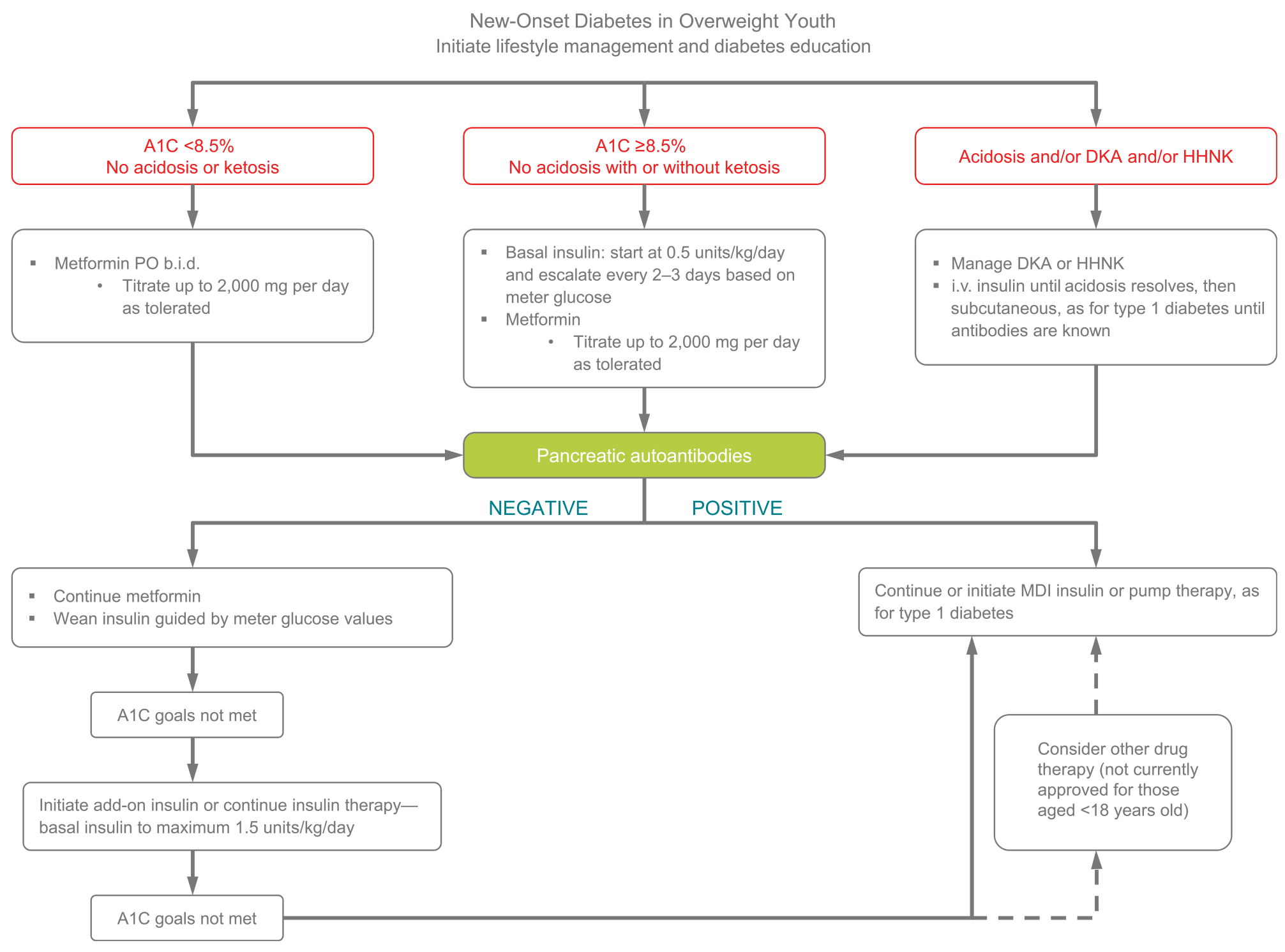
Treatment of youth-onset type 2 diabetes should include lifestyle management, diabetes self-management education, and pharmacologic treatment. Initial treatment of youth with obesity and diabetes must take into account that diabetes type is often uncertain in the first few weeks of treatment, due to overlap in presentation, and that a substantial percentage of youth with type 2 diabetes will present with clinically significant ketoacidosis (138). Therefore, initial therapy should address the hyperglycemia and associated metabolic derangements irrespective of ultimate diabetes type, with adjustment of therapy once metabolic compensation has been established and subsequent information, such as islet autoantibody results, becomes available. Figure 13.1 provides an approach to initial treatment of new-onset diabetes in overweight youth.
Glycemic targets should be individualized, taking into consideration long-term health benefits of more stringent targets as well as risk for adverse effects, such as hypoglycemia. A lower target A1C in youth with type 2 diabetes when compared with those recommended in type 1 diabetes is justified by lower risk of hypoglycemia and higher risk of complications (139-142).
Patients and their families must prioritize lifestyle modifications such as eating a balanced diet, achieving and maintaining a healthy weight, and exercising regularly. A family-centered approach to nutrition and lifestyle modi- fication is essential in children with type 2 diabetes, and nutition recommendations should be culturally appropriate and sensitive to family resources (see Section “Lifestyle Management”). Given the complex social and environmental context surrounding youth with type 2 diabetes, individual-level lifestyle interventions may not be sufficient to target the complex interplay of family dynamics, mental health, community readiness, and the broader environmental system (2).
A multidisciplinary diabetes team, including a physician, diabetes nurse educator, registered dietitian, and psychologist or social worker, is essential. In addition to blood glucose control and self-management education (143-145), initial treatment must include management of comorbidities such as obesity, dyslipidemia, hypertension, and microvascular complications.
Current pharmacologic treatment options for youth-onset type 2 diabetes are limited to two approved drugsdinsulin and metformin (2). Presentation with ketoacidosis or marked ketosis requires a period of insulin therapy until fasting and postprandial glycemia have been restored to normal or near-normal levels. Metformin therapy may be used as an adjunct after resolution of ketosis/ ketoacidosis. Initial treatment should also be with insulin when the distinction between type 1 diabetes and type 2 diabetes is unclear and in patients who have random blood glucose concentrations ≥250 mg/dL (13.9 mmol/L) and/or A1C ≥8.5% (69 mmol/mol) (146). Insulin is needed when the glycemic target is not met on metformin alone, or if there is metformin intolerance or renal or hepatic insufficiency (147).
When insulin treatment is not required, initiation of metformin is recommended. The Treatment Options for Type 2 Diabetes in Adolescents and Youth (TODAY) study found that metformin alone provided durable glycemic control (A1C ≤8% [64 mmol/mol] for 6 months) in approximately half of the subjects (148). To date, the TODAY study is the only trial combining lifestyle and metformin therapy in youth with type 2 diabetes; the combination did not perform better than metformin alone in achieving durable glycemic control (148).