4.2.0.0 Overview
The care of older adults with diabetes is complicated by their clinical, cognitive, and functional heterogeneity. Some older individuals may have developed diabetes years earlier and have signifi- cant complications, others are newly diagnosed and may have had years of undiagnosed diabetes with resultant complications, and still other older adults may have truly recent-onset disease with few or no complications (22). Some older adults with diabetes have other underlying chronic conditions, substantial diabetes-related comorbidity, limited cognitive or physical functioning, or frailty (23,24). Other older individuals with diabetes have little comorbidity and are active. Life expectancies are highly variable but are often longer than clinicians realize. Providers caring for older adults with diabetes must take this heterogeneity into consideration when setting and prioritizing treatment goals (25) (Table 12.1). In addition, older adults with diabetes should be assessed for disease treatment and self-management knowledge, health literacy, and mathematical literacy (numeracy) at the onset of treatment. See Fig. 6.1 for patient- and disease-related factors to consider when determining individualized glycemic targets.
A1C is used as the standard biomarker for glycemic control in all patients with diabetes but may have limitations in patients who have medical conditions that impact red blood cell turnover (see Section 2 “Classification and Diagnosis of Diabetes” for additional details on the limitations of A1C) (26). Many conditions associated with increased red blood cell turnover, such as hemodialysis, recent blood loss or transfusion, or erythropoietin therapy, are commonly seen in older adults with functional limitations, which can falsely increase or decrease A1C. In these instances, plasma blood glucose and fingerstick readings should be used for goal setting (Table 12.1).
Table 12.1—Framework for considering treatment goals for glycemia, blood pressure, and dyslipidemia in older adults with diabetes (2)
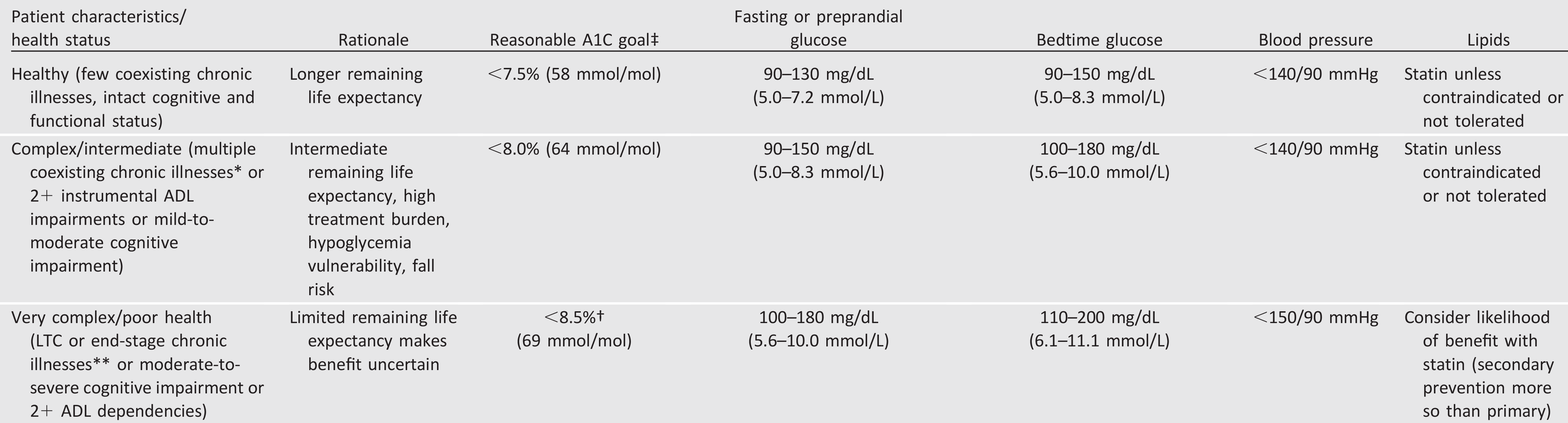
This represents a consensus framework for considering treatment goals for glycemia, blood pressure, and dyslipidemia in older adults with diabetes. The patient characteristic categories are general concepts. Not every patient will clearly fall into a particular category. Consideration of patient and caregiver preferences is an important aspect of treatment individualization. Additionally, a patient’s health status and preferences may change over time.
‡A lower A1C goal may be set for an individual if achievable without recurrent or severe hypoglycemia or undue treatment burden.
*Coexisting chronic illnesses are conditions serious enough to require medications or lifestyle management and may include arthritis, cancer, congestive heart failure, depression, emphysema, falls, hypertension, incontinence, stage 3 or worse chronic kidney disease, myocardial infarction, and stroke.“Multiple” means at least three, but many patients may have five or more (54).
**The presence of a single end-stage chronic illness, such as stage 3-4 congestive heart failure or oxygen-dependent lung disease, chronic kidney disease requiring dialysis, or uncontrolled metastatic cancer, may cause significant symptoms or impairment of functional status and significantly reduce life expectancy.
†A1C of 8.5% (69 mmol/mol) equates to an estimated average glucose of ~200 mg/dL (11.1 mmol/L). Looser A1C targets above 8.5% (69 mmol/mol) are not recommended as they may expose patients to more frequent higher glucose values and the acute risks from glycosuria, dehydration, hyperglycemic hyperosmolar syndrome, and poor wound healing. ADL, activities of daily living.