2.4.0.0 Treatment Strategies
2.4.1.0 Lifestyle Intervention
Recommendations
10.7 For patients with blood pressure >120/80 mmHg, lifestyle intervention consists of weight loss if overweight or obese, a Dietary Approaches to Stop Hypertension (DASH)-style dietary pattern including reducing sodium and increasing potassium intake, moderation of alcohol intake, and increased physical activity. B
Lifestyle management is an important component of hypertension treatment because it lowers blood pressure, enhances the effectiveness of some antihypertensive medications, promotes other aspects of metabolic and vascular health, and generally leads to few adverse effects. Lifestyle therapy consists of reducing excess body weight through caloric restriction, restricting sodium intake (<2,300 mg/day), increasing consumption of fruits and vegetables (8–10 servings per day) and low-fat dairy products (2–3 servings per day), avoiding excessive alcohol consumption (no more than 2 servings per day in men and no more than 1 serving per day in women) (46), and increasing activity levels (47).
These lifestyle interventions are reasonable for individuals with diabetes and mildly elevated blood pressure (systolic >120 mmHg or diastolic >80 mmHg) and should be initiated along with pharmacologic therapy when hypertension is diagnosed (Fig. 10.1) (47). A lifestyle therapy plan should be developed in collaboration with the patient and discussed as part of diabetes management.
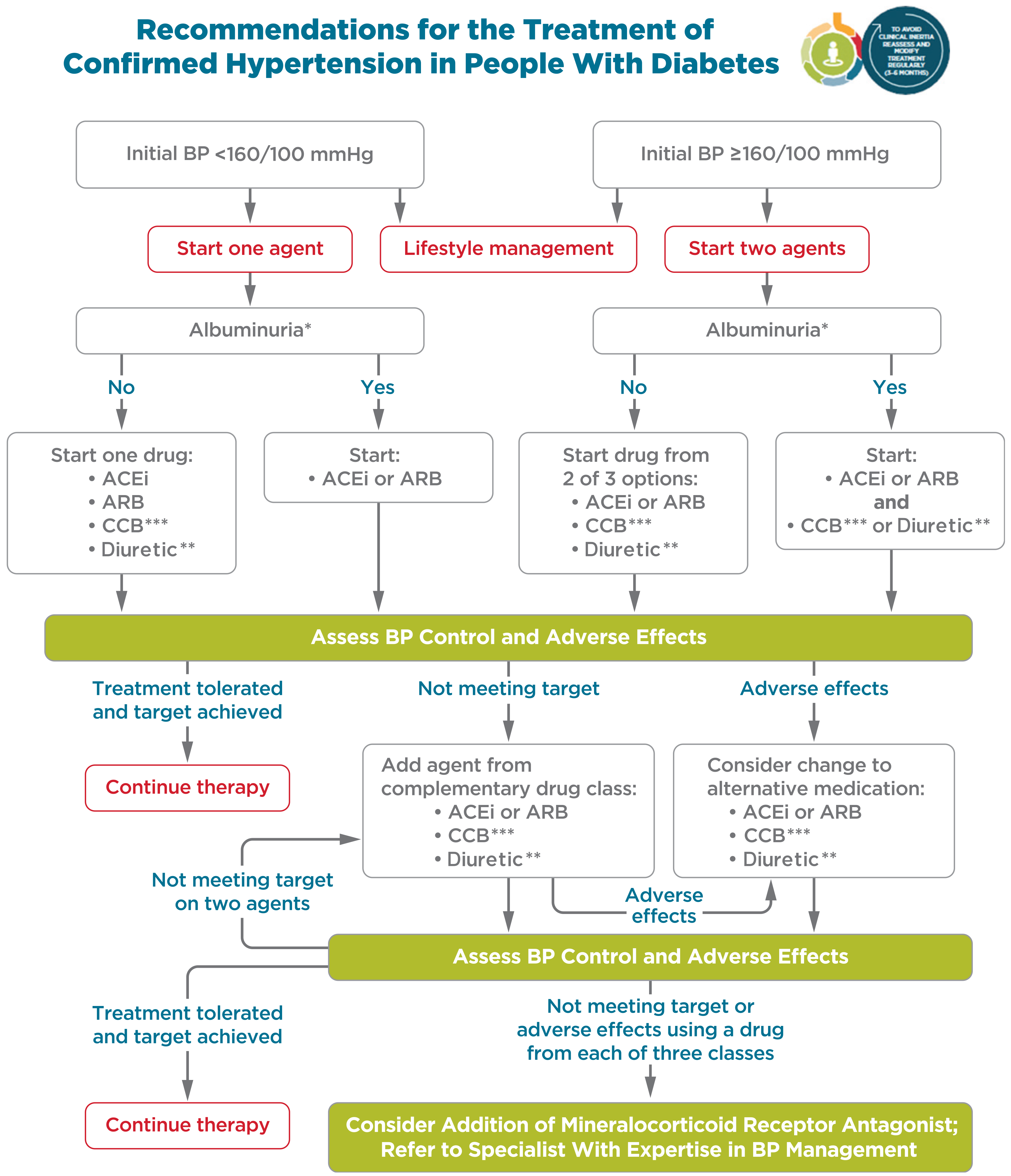
Figure 10.1—Recommendations for the treatment of confirmed hypertension in people with diabetes
Figure 10.1—Recommendations for the treatment of confirmed hypertension in people with diabetes.
*An ACE inhibitor (ACEi) or angiotensin receptor blocker (ARB) is suggested to treat hypertension for patients with urine albumin-to-creatinine ratio 30–299 mg/g creatinine and strongly recommended for patients with urine albumin-to-creatinine ratio ≥300 mg/g creatinine.
**Thiazide-like diuretic; long-acting agents shown to reduce cardiovascular events, such as chlorthalidone and indapamide, are preferred.
***Dihydropyridine calcium channel blocker (CCB). BP, blood pressure. Adapted from de Boer et al. (17).
For interactive tool, see here