
Guideline 8
7. Diabetes Technology: Standards of Medical Care in Diabetes–2019
The American Diabetes Association (ADA) “Standards of Medical Care in Diabetes” includes ADA’s current clinical practice recommendations and is intended to provide the components of diabetes care, general treatment goals and guidelines, and tools to evaluate quality of care. Members of the ADA Professional Practice Committee, a multidisciplinary expert committee, are responsible for updating the Standards of Care annually, or more frequently as warranted. For a detailed description of ADA standards, statements, and reports, as well as the evidence-grading system for ADA’s clinical practice recommendations, please refer to the Standards of Care Introduction. Readers who wish to comment on the Standards of Care are invited to do so at professional.diabetes.org/SOC.
Diabetes technology is the term used to describe the hardware, devices, and software that people with diabetes use to help manage blood glucose levels, stave off diabetes complications, reduce the burden of living with diabetes, and improve quality of life. Historically, diabetes technology has been divided into two main categories: insulin administered by syringe, pen, or pump, and blood glucose monitoring as assessed by meter or continuous glucose monitor. More recently, diabetes technology has expanded to include hybrid devices that both monitor glucose and deliver insulin, some automatically, as well as software that serves as a medical device, providing diabetes self-management support. Diabetes technology, when applied appropriately, can improve the lives and health of people with diabetes; however, the complexity and rapid change of the diabetes technology landscape can also be a barrier to patient and provider implementation.
To provide some additional clarity in the diabetes technology space, the American Diabetes Association is, for the first time, adding a dedicated section on diabetes technology to the “Standards of Medical Care in Diabetes.” For this first writing, the section will focus on insulin delivery and glucose monitoring with the most common devices currently in use. In future years, this section will be expanded to include software as a medical device, privacy, cost, technology-enabled diabetes education and support, telemedicine, and other issues that providers and patients encounter with the use of technology in modern diabetes care.
Suggested citation: American Diabetes Association.
7. Diabetes technology: Standards of Medical
Care in Diabetesd2019. Diabetes Care 2019;42
(Suppl. 1):S71–S80
© 2018 by the American Diabetes Association.
Readers may use this article as long as the work
is properly cited, the use is educational and not
for profit, and the work is not altered. More information
is available at http://www.diabetesjournals
.org/content/license.
2.0.0.0 INSULIN DELIVERY
2.1.0.0 Insulin Syringes and Pens
Recommendations
7.1 For people with diabetes who require insulin, insulin syringes or insulin pens may be used for insulin delivery with consideration of patient preference, insulin type and dosing regimen, cost, and self-management capabilities. B
7.2 Insulin pens or insulin injection aids may be considered for patients with dexterity issues or vision impairment to facilitate the administration of accurate insulin doses. C
Injecting insulin with a syringe or pen is the insulin delivery method used by most people with diabetes (1,2), with the remainder using insulin pumps or automated insulin delivery devices (see sections on those topics below). For patients with diabetes who use insulin, insulin syringes and pens are both able to deliver insulin safely and effectively for the achievement of glycemic targets. When choosing between a syringe and a pen, patient preferences, cost, insulin type and dosing regimen, and self-management capabilities should be considered. It is important to note that while many insulin types are available for purchase as either pens or vials, others may only be available in one form or the other and there may be significant cost differences between pens and vials (see Table 9.3 for a list of insulin product costs with dosage forms). Insulin pens may allow people with vision impairment or dexterity issues to dose insulin accurately (3–5), while insulin injection aids are also available to help with these issues (http://main.diabetes.org/dforg/pdfs/2018/2018-cg-injection-aids.pdf).
The most common syringe sizes are 1 mL, 0.5 mL, and 0.3 mL, allowing doses of up to 100 units, 50 units, and 30 units of U-100 insulin, respectively. In a few parts of the world, insulin syringes still have U-80 and U-40 markings for older insulin concentrations and veterinary insulin, and U-500 syringes are available for the use of U-500 insulin. Syringes are generally used once but may be reused by the same individual in resource-limited settings with appropriate storage and cleansing (6).
Insulin pens offer added convenience by combining the vial and syringe into a single device. Insulin pens, allowing push-button injections, come as disposable pens with prefilled cartridges or reusable insulin pens with replaceable insulin cartridges. Some reusable pens include a memory function, which can recall dose amounts and timing. “Smart” pens that can be programmed to calculate insulin doses and provide downloadable data reports are also available. Pens also vary with respect to dosing increment and minimal dose, which can range from half-unit doses to 2-unit dose increments.
Needle thickness (gauge) and length is another consideration. Needle gauges range from 22 to 33, with higher gauge indicating a thinner needle. A thicker needle can give a dose of insulin more quickly, while a thinner needle may cause less pain. Needle length ranges from 4 to 12.7 mm, with some evidence suggesting shorter needles may lower the risk of intramuscular injection. When reused, needles may be duller and thus injection more painful. Proper insulin technique is a requisite to obtain the full benefits of insulin injection therapy, and concerns with technique and using the proper technique are outlined in Section 9 “Pharmacologic Approaches to Glycemic Treatment.”
Another insulin delivery option is a disposable patch-like device, which provides a continuous, subcutaneous infusion of rapid-acting insulin (basal), as well as 2-unit increments of bolus insulin at the press of a button (7).
2.2.0.0 Insulin Pumps
Recommendations
7.3 Individuals with diabetes who have been successfully using continuous subcutaneous insulin infusion should have continued access across third-party payers. E
7.4 Most adults, children, and adolescents with type 1 diabetes should be treated with intensive insulin therapy with either multiple daily injections or an insulin pump. A
7.5 Insulin pump therapy may be considered as an option for all children and adolescents, especially in children under 7 years of age. C
Continuous subcutaneous insulin injection (CSII) or insulin pumps have been available in the U.S. for 40 years. These devices deliver rapid-acting insulin throughout the day to help manage blood glucose levels. Most insulin pumps use tubing to deliver insulin through a cannula, while a few attach directly to the skin, without tubing.
Most studies comparing multiple daily injections (MDI) with CSII have been relatively small and of short duration. However, a recent systematic review and meta-analysis concluded that pump therapy has modest advantages for lowering A1C (–0.30% 95% CI -0.58 to -0.02]) and for reducing severe hypoglycemia rates in children and adults (8). There is no consensus to guide choosing which form of insulin administration is best for a given patient, and research to guide this decision making is needed (9). Thus, the choice of MDI or an insulin pump is often based upon the individual characteristics of the patient and which is most likely to benefit him or her. Newer systems, such as sensor-augmented pumps and automatic insulin delivery systems, are discussed elsewhere in this section.
Adoption of pump therapy in the U.S. shows geographical variations, which may be related to provider preference or center characteristics (10,11) and socioeconomic status, as pump therapy is more common in individuals of higher socioeconomic status as reflected by race/ethnicity, private health insurance, family income, and education (11,12). Given the additional barriers to optimal diabetes care observed in disadvantaged groups (13), addressing the differences in access to insulin pumps and other diabetes technology may contribute to fewer health disparities.
Pump therapy can be successfully started at the time of diagnosis (14,15). Practical aspects of pump therapy initiation include: assessment of patient and family readiness, (although there is no consensus on which factors to consider in adults (16) or pediatrics), selection of pump type and initial pump settings, patient/ family education of potential pump complications (e.g., diabetic ketoacidosis [DKA] with infusion set failure), transition from MDI, and introduction of advanced pump settings (e.g., temporary basal rates, extended/square/dual wave bolus).
Complications of the pump can be caused by issues with infusion sets (dislodgement, occlusion), which place patients at risk for ketosis and DKA and thus must be recognized and managed early (17); lipohypertrophy or, less frequently, lipoatrophy (18,19); and pump site infection (20). Discontinuation of pump therapy is relatively uncommon today; the frequency has decreased over the past decades and its causes have changed (20,21). Current reasons for attrition are problems with cost, wearability, disliking the pump, suboptimal glycemic control, or mood disorders (e.g., anxiety or depression) (22).
2.2.0.0 Insulin Pumps in Pediatrics
The safety of insulin pumps in youth has been established for over 15 years (23). Studying the effectiveness of CSII in lowering A1C has been challenging because of the potential selection bias of observational studies. Participants on CSII may have a higher socioeconomic status that may facilitate better glycemic control (24) versus MDI. In addition, the fast pace of development of new insulins and technologies quickly renders comparisons obsolete. However, randomized controlled trials (RCTs) comparing CSII and MDI with insulin analogs demonstrate a modest improvement in A1C in participants on CSII (25,26). Observational studies, registry data, and meta-analysis have also suggested an improvement of glycemic control in participants on CSII (27–29). Although hypoglycemia was a major adverse effect of intensified insulin regimen in the Diabetes Control and Complications Trial (DCCT) (30), data suggests that CSII may reduce the rates of severe hypoglycemia compared with MDI (29,31–33). There is also evidence that CSII may reduce DKA risk (29,34) and diabetes complications, in particular, retinopathy and peripheral neuropathy in youth, compared with MDI (35). Finally, treatment satisfaction and quality-of-life measures improved on CSII compared with MDI (36,37). Therefore, CSII can be used safely and effectively in youth with type 1 diabetes to assist with achieving targeted glycemic control while reducing the risk of hypoglycemia and DKA, improving quality of life and preventing long-term complications. Based on patient-provider shared decision making, insulin pumps may be considered in all pediatric patients. In particular, pump therapy may be the preferred mode of insulin delivery for children under 7 years of age (38). Because of a paucity of data in adolescents and youths with Type 2 diabetes, there is insufficient evidence to make recommendations.
Common barriers to pump therapy adoption in children and adolescents are concerns regarding the physical interference of the device, discomfort with idea of having a device on the body therapeutic effectiveness, and financial burden (27,39).
3.0.0.0 SELF-MONITORING OF BLOOD GLUCOSE
3.1.0.0 Introduction
Recommendations
7.6 Most patients using intensive insulin regimens (multiple daily injections or insulin pump therapy) should assess glucose levels using self-monitoring of blood glucose (or continuous glucose monitoring) prior to meals and snacks, at bedtime, occasionally postprandially, prior to exercise, when they suspect low blood glucose, after treating low blood glucose until they are normoglycemic, and prior to critical tasks such as driving. B
7.7 When prescribed as part of a broad educational program, self-monitoring of blood glucose may help to guide treatment decisions and/or self-management for patients taking less frequent insulin injections. B
7.8 When prescribing self-monitoring of blood glucose, ensure that patients receive ongoing instruction and regular evaluation of technique, results, and their ability to use data from self-monitoring of blood glucose to adjust therapy. Similarly, continuous glucose monitoring use requires robust and ongoing diabetes education, training, and support. E
Major clinical trials of insulin-treated patients have included self-monitoring of blood glucose (SMBG) as part of multifactorial interventions to demonstrate the benefit of intensive glycemic control on diabetes complications (40). SMBG is thus an integral component of effective therapy of patients taking insulin. In recent years, continuous glucose monitoring (CGM) has emerged as a complementary method for the assessment of glucose levels (discussed below). Glucose monitoring allows patients to evaluate their individual response to therapy and assess whether glycemic targets are being safely achieved. Integrating results into diabetes management can be a useful tool for guiding medical nutrition therapy and physical activity, preventing hypoglycemia, and adjusting medications (particularly prandial insulin doses). The patient’s specific needs and goals should dictate SMBG frequency and timing or the consideration of CGM use.
3.2.0.0 Optimizing Self-monitoring of Blood Glucose and Continuous Glucose Monitor Use
SMBG and CGM accuracy is dependent on the instrument and user, so it is important to evaluate each patient’s monitoring technique, both initially and at regular intervals thereafter. Optimal use of SMBG and CGM requires proper review and interpretation of the data, by both the patient and the provider, to ensure that data are used in an effective and timely manner. For patients with type 1 diabetes using CGM, the greatest predictor of A1C lowering for all age-groups was frequency of sensor use, which was highest in those aged ≥25 years and lower in younger age-groups (41). Similarly, for SMBG in patients with type 1 diabetes, there is a correlation between greater SMBG frequency and lower A1C (42). Among patients who check their blood glucose at least once daily, many report taking no action when results are high or low (43). Patients should be taught how to use SMBG and/or CGM data to adjust food intake, exercise, or pharmacologic therapy to achieve specific goals. The ongoing need for and frequency of SMBG should be reevaluated at each routine visit to avoid overuse, particularly if SMBG is not being used effectively for self-management (43–45).
3.3.0.0 For Patients on Intensive Insulin Regimens
SMBG or CGM is especially important for insulin-treated patients to monitor for and prevent hypoglycemia and hyperglycemia. Most patients using intensive insulin regimens (MDI or insulin pump therapy) should assess glucose levels using SMBG or a CGM prior to meals and snacks, at bedtime, occasionally postprandially, prior to exercise, when they suspect low blood glucose, after treating low blood glucose until they are normoglycemic, and prior to critical tasks such as driving. For many patients using SMBG, this will require testing up to 6–10 times daily, although individual needs may vary. A database study of almost 27,000 children and adolescents with type 1 diabetes showed that, after adjustment for multiple confounders, increased daily frequency of SMBG was significantly associated with lower A1C (–0.2% per additional test per day) and with fewer acute complications (46).
3.4.0.0 For Patients Using Basal Insulin and/or Oral Agents
The evidence is insufficient regarding when to prescribe SMBG and how often testing is needed for insulin-treated patients who do not use intensive insulin regimens, such as those with type 2 diabetes using basal insulin with or without oral agents. However, for patients using basal insulin, assessing fasting glucose with SMBG to inform dose adjustments to achieve blood glucose targets results in lower A1C (47,48).
In people with type 2 diabetes not using insulin, routine glucose monitoring may be of limited additional clinical benefit. For some individuals, glucose monitoring can provide insight into the impact of diet, physical activity, and medication management on glucose levels. Glucose monitoring may also be useful in assessing hypoglycemia, glucose levels during intercurrent illness, or discrepancies between measured A1C and glucose levels when there is concern an A1C result may not be reliable in specific individuals. However, several randomized trials have called into question the clinical utility and cost-effectiveness of routine SMBG in noninsulin-treated patients (49–52). In a year-long study of insulin-naive patients with suboptimal initial glycemic control, a group trained in structured SMBG (a paper tool was used at least quarterly to collect and interpret seven-point SMBG profiles taken on 3 consecutive days) reduced their A1C by 0.3% more than the control group (53). A trial of once-daily SMBG that included enhanced patient feedback through messaging found no clinically or statistically significant change in A1C at 1 year (52). Meta-analyses have suggested that SMBG can reduce A1C by 0.25–0.3% at 6 months (54–56), but the effect was attenuated at 12 months in one analysis (54). Reductions in A1C were greater (20.3%) in trials where structured SMBG data were used to adjust medications but not significant without such structured diabetes therapy adjustment (56). A key consideration is that performing SMBG alone does not lower blood glucose levels. To be useful, the information must be integrated into clinical and self-management plans.
3.5.0.0 Glucose Meter Accuracy
Recommendation
7.9 Health care providers should be aware of the medications and other factors that can interfere with glucose meter accuracy and choose appropriate devices for their patients based on these factors. E
Glucose meters meeting U.S. Food and Drug Administration (FDA) guidance for meter accuracy provide the most reliable data for diabetes management. There are several current standards for accuracy of blood glucose monitors, but the two most used are those of the International Organization for Standardization (ISO 15197:2013) and the FDA. The current ISO and FDA standards are compared in Table 7.1. In Europe, currently marketed monitors must meet current ISO standards. In the U.S., currently marketed monitors must meet the standard under which they were approved, which may not be the current standard. Moreover, the monitoring of current accuracy is left to the manufacturer and not routinely checked by an independent source.
Patients assume their glucose monitor is accurate because it is FDA cleared, but often that is not the case. There is substantial variation in the accuracy of widely used blood glucose monitoring systems. The Diabetes Technology Society Blood Glucose Monitoring System Surveillance Program provides information on the performance of devices used for SMBG (https://www.diabetestechnology.org/surveillance.shtml). In a recent analysis, theprogram found that only 6 of the top 18 glucose meters met the accuracy standard (57).
Factors Limiting Accuracy
Counterfeit Strips. Patients should be advised against purchasing or reselling preowned or second-hand test strips, as these may give incorrect results. Only unopened vials of glucose test strips should be used to ensure SMBG accuracy.
Oxygen. Currently available glucose monitors utilize an enzymatic reaction linked to an electrochemical reaction, either glucose oxidase or glucose dehydrogenase (58). Glucose oxidase monitors are sensitive to the oxygen available and should only be used with capillary blood in patients with normal oxygen saturation. Higher oxygen tensions (i.e., arterial blood or oxygen therapy) may result in false low-glucose readings, and low oxygen tensions (i.e., high altitude, hypoxia, or venous blood readings) may lead to false high-glucose readings. Glucose dehydrogenase monitors are not sensitive to oxygen.
Temperature. Because the reaction is sensitive to temperature, all monitors have an acceptable temperature range (58). Most will show an error if the temperature is unacceptable, but a few will provide a reading and a message indicating that the value may be incorrect.
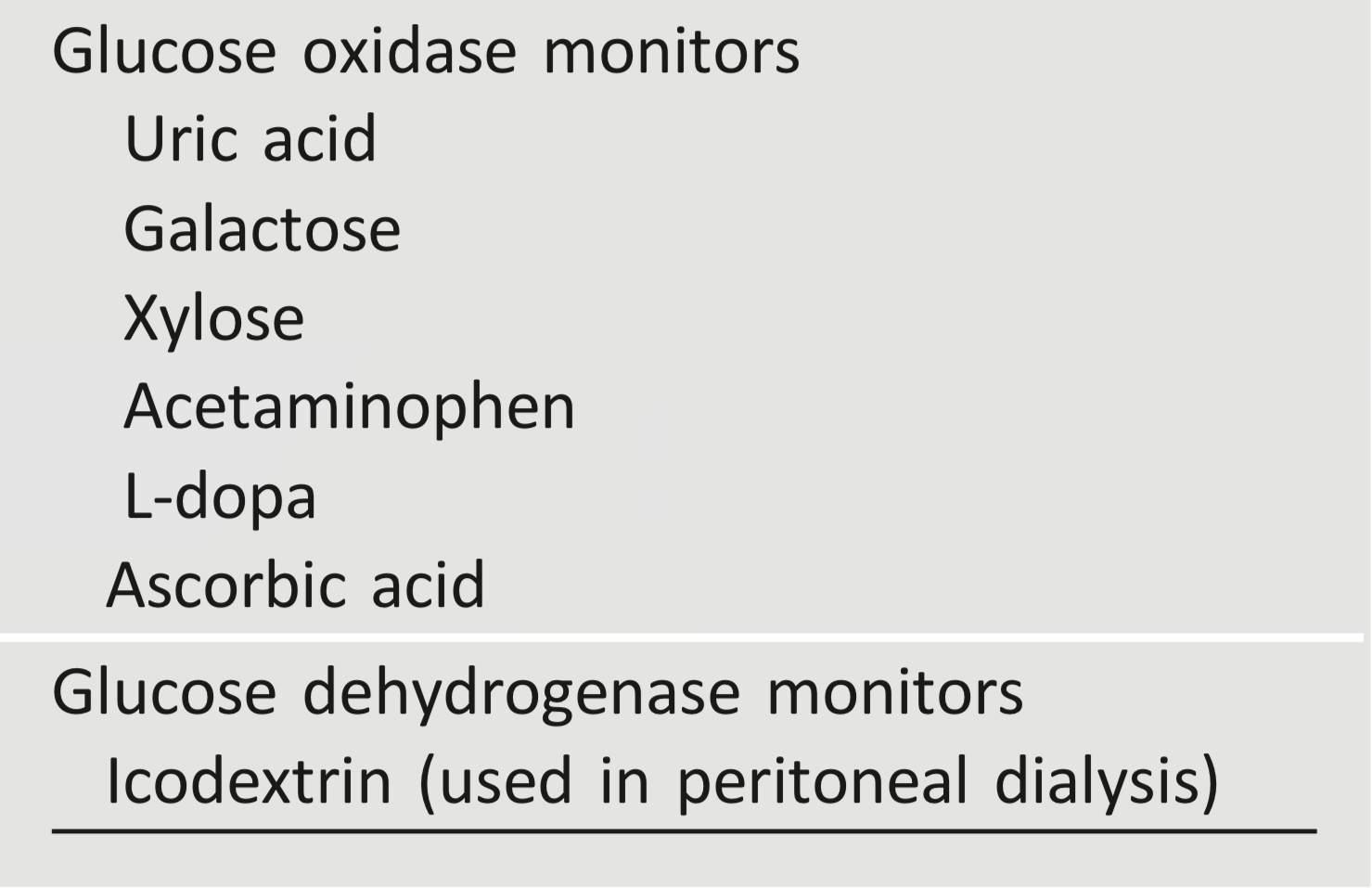
Interfering Substances. There are a few physiologic and pharmacologic factors that interfere with glucose readings. Most interfere only with glucose oxidase systems (58). They are listed in Table 7.2.
Table 7.1—Comparison of ISO 15197 and FDA blood glucose meter accuracy standards
Table 7.2—Interfering substances
4.0.0.0 CONTINUOUS GLUCOSE MONITORS
4.1.0.0 Introduction
Recommendations
7.10 Sensor-augmented pump therapy may be considered for children, adolescents, and adults to improve glycemic control without an increase in hypoglycemia or severe hypoglycemia. Benefits correlate with adherence to ongoing use of the device. A
7.11 When prescribing continuous glucose monitoring, robust diabetes education, training, and support are required for optimal continuous glucose monitor implementation and ongoing use. E
7.12 People who have been successfully using continuous glucose monitors should have continued access across third-party payers. E
CGM measures interstitial glucose (which correlates well with plasma glucose). There are two types of CGM devices. Most CGM devices are real-time CGM, which continuously report glucose levels and include alarms for hypoglycemic and hyperglycemic excursions. The other type of device is intermittently scanning CGM (isCGM), which is approved for adult use only. isCGM, discussed more fully below, does not have alarms and does not communicate continuously, only on demand. It is reported to have a lower cost than systems with automatic alerts.
For some CGM systems, SMBG is required to make treatment decisions, although a randomized controlled trial of 226 adults suggested that an enhanced CGM device could be used safely and effectively without regular confirmatory SMBG in patients with well-controlled type 1 diabetes at low risk of severe hypoglycemia (59). Two CGM devices are now approved by the FDA for making treatment decisions without SMBG confirmation, sometimes called adjunctive use (60,61).
The abundance of data provided by CGM offers opportunities to analyze patient data more granularly than was previously possible, providing additional information to aid in achieving glycemic targets. A variety of metrics have been proposed (62). As recently reported, the metrics may include: 1) average glucose; 2) percentage of time in hypoglycemic ranges, i.e., <54 mg/dL (level 2), 54–70 mg/dL (level 1) (62); 3) percentage of time in target range, i.e., 70–180 mg/dL (3.9–9.9 mmol/L); 4) percentage of time in hyperglycemic range, i.e., ≥180 mg/dL (62). To make these metrics more actionable, standardized reports with visual cues, such as an ambulatory glucose profile (62), may help the patient and the provider interpret the data and use it to guide treatment decisions.
In addition, while A1C is well established as an important risk marker for diabetes complications, with the increasing use of CGM to help facilitate safe and effective diabetes management, it is important to understand how CGM metrics, such as mean glucose and A1C correlate. Estimated A1C (eA1C) is a measure converting the mean glucose from CGM or self-monitored blood glucose readings, using a formula derived from glucose readings from a population of individuals, into an estimate of a simultaneously measured laboratory A1C. Recently, the eA1C was renamed the glucose management indicator (GMI), and a new formula was generated for converting CGM-derived mean glucose to GMI based on recent clinical trials using the most accurate CGM systems available. This provided a new way to use CGM data to estimate A1C (63).
4.2.0.0 Real-time Continuous Glucose Monitor Use in Youth
Recommendation
7.13 Real-time continuous glucose monitoring should be considered in children and adolescents with type 1 diabetes, whether using multiple daily injections or continuous subcutaneous insulin infusion, as an additional tool to help improve glucose control and reduce the risk of hypoglycemia. Benefits of continuous glucose monitoring correlate with adherence to ongoing use of the device. B
Data regarding use of real-time CGM in youth consist of findings from RCTs and small observational studies, as well as analysis of data collected by registries. Some of the RCTs have included both adult and pediatric participants (41,64–66), while others have only included pediatric participants (67) or limited the analysis of larger studies to just the pediatric participants (41). Given the feasibility problems of performing RCTs in very young children, small observational studies have also provided data on real-time CGM use in the youngest age groups (68–70). Finally, while limited by the observational nature, registry data provide some evidence of real-world use of the technologies (71,72).
Impact on Glycemic Control
When data from adult and pediatric participants is analyzed together, CGM use in RCTs has been associated with reduction in A1C levels (64–66). Yet, in the JDRF CGM trial, when youth were analyzed by age-group (8- to 14-year-olds and 15- to 24-year-olds), no change in A1C was seen, likely due to poor CGM adherence (41). Indeed, in a secondary analysis of that RCT’s data in both pediatric cohorts, those who utilized the sensor ≥6 days/week had an improvement in their glycemic control (73). One critical component to success with CGM is near-daily wearing of the device (64,74–76).
Though data from small observational studies demonstrate that CGM can be worn by patients <8 years old and the use of CGM provides insight to glycemic patterns (68,69), an RCT in children aged 4 to 9 years did not demonstrate improvements in glycemic control following 6 months of CGM use (67). However, observational feasibility studies of toddlers demonstrated a high degree of parental satisfaction and sustained use of the devices despite the inability to change the degree of glycemic control attained (70).
Registry data has also shown an association between CGM use and lower A1C levels (71,72), even when limiting assessment of CGM use to participants on injection therapy (72).
Impact on Hypoglycemia
Apart from the Sensing With Insulin pump Therapy to Control HbA1c (SWITCH) study, which showed a significant effect of adding CGM to insulin pump therapy on time spent in hypoglycemia (64), most studies focusing on glycemic management overall failed to demonstrate a significant or relevant reduction in level 1 hypoglycemia (41,65– 67,77). Notably, RCTs primarily aimed at hypoglycemia prevention did demonstrate a significant reduction in mild hypoglycemia in terms of reducing the time spent in hypoglycemia by approximately 40% and reducing the number of level 1 hypoglycemia events per day (78,79).
4.3.0.0 Real-time Continuous Glucose Monitor Use in Adults
Recommendations
7.14 When used properly, real-time continuous glucose monitoring in conjunction with intensive insulin regimens is a useful tool to lower A1C in adults with type 1 diabetes who are not meeting glycemic targets. A
7.15 Real-time continuous glucose monitoring may be a useful tool in those with hypoglycemia unawareness and/or frequent hypoglycemic episodes. B
7.16 Real-time continuous glucose monitoring should be used as close to daily as possible for maximal benefit. A
7.17 Real-time continuous glucose monitoring may be used effectively to improve A1C levels and neonatal outcomes in pregnant women with type 1 diabetes. B
7.18 Sensor-augmented pump therapy with automatic low-glucose suspend may be considered for adults with type 1 diabetes at high risk of hypoglycemia to prevent episodes of hypoglycemia and reduce their severity. B
Data exist to support the use of CGM in adults, both those on MDI and on CSII. In terms of randomized controlled trials in people with type 1 diabetes, there are four studies in adults with A1C as the primary outcome (80–84), three studies in adults with hypoglycemia as the primary outcome (85–87), four studies in adults and children with A1C as the primary outcome (41,64–66), and three studies in adults and children with hypoglycemia as a primary outcome (41,78,,88). There are three studies in adults with type 1 or type 2 diabetes (89–91) and four studies with adults with type 2 diabetes (92–95). Finally, there are three studies that have been done in pregnant women with prepregnancy diabetes or gestational diabetes mellitus (96–98). Overall, excluding studies evaluating pediatric patients alone or pregnant women, 2,984 people with type 1 or type 2 diabetes have been studied to assess the benefits of CGM.
Primary Outcome: A1C Reduction
In general, A1C reduction was shown in studies where the baseline A1C was higher. In two larger studies in adults with type 1 diabetes that assessed the benefit of CGM in patients on MDI, there were significant reductions in A1C: -0.6% in one (80,81) and -0.43% in the other (82). No reduction in A1C was seen in a small study performed in underserved, less well-educated adults with type 1 diabetes (83). In the adult subset of the JDRF CGM study, there was a significant reduction in A1C of -0.53% (71) in patients who were primarily treated with insulin pump therapy. Better adherence in wearing the CGM device resulted in a greater likelihood of an improvement in glycemic control (41,84).
Studies in people with type 2 diabetes are heterogeneous in designdin two, participants were using basal insulin with oral agents or oral agents alone (65,95); in one, individuals were on MDI alone (92); and in another, participants were on CSII or MDI (79). The findings in studies with MDI alone (92) and in two studies in people using oral agents with or without insulin (93,95) showed significant reductions in A1C levels.
Primary Outcome: Hypoglycemia
In studies in adults where reduction in episodes of hypoglycemia was the primary end point, significant reductions were seen in individuals with type 1 diabetes on MDI or CSII (85–87). In one study in patients who were at higher risk for episodes of hypoglycemia (87), there was a reduction in rates of all levels of hypoglycemia (see Section 6 “Glycemic Targets” for hypoglycemia definitions). The Multiple Daily Injections and Continuous Glucose Monitoring in Diabetes (DIAMOND) study in people with type 2 diabetes on MDI did not show a reduction in hypoglycemia (92). Studies in individuals with type 2 diabetes on oral agents with or without insulin did not show reductions in rates of hypoglycemia (93,95). CGM may be particularly useful in insulin-treated patients with hypoglycemia unawareness and/or frequent hypoglycemic episodes, although studies have not shown consistent reductions in severe hypoglycemia (41,64,,65).
Sensor-augmented pumps that suspend insulin when glucose is low or predicted to go low within the next 30 min have been approved by the FDA. The Automation to Simulate Pancreatic Insulin Response (ASPIRE) trial of 247 patients with type 1 diabetes and documented nocturnal hypoglycemia showed that sensor-augmented insulin pump therapy with a low-glucose suspend function significantly reduced nocturnal hypoglycemia over 3 months without increasing A1C levels (66). In a different sensor-augmented pump, predictive low-glucose suspend reduced time spent with glucose <70 mg/dL from 3.6% at baseline to 2.6% (3.2% with sensor-augmented pump therapy without predictive low glucose suspend) without rebound hyperglycemia during a 6-week randomized crossover trial (95a). These devices may offer the opportunity to reduce hypoglycemia for those with a history of nocturnal hypoglycemia.
4.4.0.0 Real-time Continuous Glucose Monitor Use in Pregnancy
One well-designed RCT showed a reduction in A1C levels in adult women with type 1 diabetes on MDI or CSII who were pregnant (96). Neonatal outcomes were better when the mother used CGM during pregnancy (80). Two studies employing intermittent use of real-time CGM showed no difference in neonatal outcomes in women with type 1 diabetes (97) or gestational diabetes mellitus (98).
4.5.0.0 Intermittently Scanned Continuous Glucose Monitor Use
Recommendation
7.19 Intermittently scanned continuous glucose monitor use may be considered as a substitute for self-monitoring of blood glucose in adults with diabetes requiring frequent glucose testing. C
isCGM (sometimes referred to as “flash” CGM) is a CGM that measures glucose in interstitial fluid through a <0.4 mm– thick filament that is inserted under the skin. It has been available in Europe since 2014 and was approved by the FDA for use in adults in the U.S. in 2017. The personal version of isCGM has a receiver that, after scanning over the sensor by the individual, displays real-time glucose values and glucose trend arrows. The data can be uploaded and a report created using available software. In the professional version, the patient does not carry a receiver; the data are blinded to the patient and the device is downloaded in the diabetes care provider’s office using the provider’s receiver and the software. The isCGM sensor is smaller than those of other systems and is water resistant. In the U.S., the FDA now requires a 1-h start-up time after activation of the system, and it can be worn up to 14 days. The isCGM does not require calibration with SMBG because it is factory calibrated. Acetaminophen does not cause interference with glucose readings. The mean absolute relative difference reported by the manufacturer is 9.4%. It measures glucose every minute, records measurements every 15 min, and displays up to 8 h of data. As opposed to real-time CGM systems, isCGM has no alarms. The direct costs of isCGM are lower than those of realtime CGM systems. In general, both the consumer and professional versions are covered by most commercial insurance carriers and eligible Medicare programs. Information on Medicaid coverage was not available at the time of this writing.
Studies in adults with diabetes indicate isCGM has acceptable accuracy when compared with SMBG (99–102), although the accuracy may be lower at high and/or low glucose levels (103,104). Studies comparing the accuracy of isCGM with real-time CGM show conflicting results (102,104,,105). isCGM may decrease the risk of hypoglycemia in individuals with type 1 (85) or type 2 diabetes (94). There are a growing number of studies suggesting similar good performance and potential for benefit in special populations, including pregnant women with diabetes (106), individuals with type 1 diabetes and hypoglycemia unawareness(107), and children (108–110), although accuracy (mean absolute relative difference) could be decreased in younger children (109). Contact dermatitis has been reported and linked to the presence of isobornyl acrylate, a structural plastic of the device, which is a skin sensitizer and can cause an additional spreading allergic reaction (111–113).
There are several published reviews of data available on isCGM (114–116). The Norwegian Institute for Public Health conducted an assessment of isCGM clinical effectiveness, cost-effectiveness, and safety for individuals with type 1 and type 2 diabetes, based on data available until January 2017 (114). The authors concluded that, although there were few quality data available at the time of the report, isCGM may increase treatment satisfaction, increase time in range, and reduce frequency of nocturnal hypoglycemia, without differences in A1C or quality of life or serious adverse events. The Canadian Agency for Drugs and Technologies in Health reviewed existing data on isCGM performance and accuracy, hypoglycemia, effect on A1C, and patient satisfaction and quality of life and concluded that the system could replace SMBG in particular in patients who require frequent testing (115). The last review published at the time of this report (116) also supported the use of isCGM as a more affordable alternative to real-time CGM systems for individuals with diabetes who are on intensive insulin therapy.
5.0.0.0 AUTOMATED INSULIN DELIVERY
Recommendation
7.20 Automated insulin delivery systems may be considered in children (>7 years) and adults with type 1 diabetes to improve glycemic control. B
To provide physiologic insulin delivery, insulin doses need to be adjusted based on glucose values, which is now feasible with automated insulin delivery systems consisting of three components: an insulin pump, a continuous glucose sensor, and an algorithm that determines insulin delivery. With these systems, insulin delivery cannot only be suspended but also increased or decreased based on sensor glucose values. Emerging evidence suggests such systems may lower the risk of exercise-related hypoglycemia (117) and may have psychosocial benefits (118–121).
While eventually insulin delivery in closed-loop systems may be truly automated, meals must currently be announced. A so-called hybrid approach, hybrid closed-loop (HCL), has been adopted in first-generation closed-loop systems and requires users to bolus for meals and snacks. The FDA has approved the first HCL system for use in those as young as 7 years of age. A 3-month noncontrolled trial using this device (n = 124) demonstrated safety (122) and improved A1C in adults (reduction from 7.3 ± 0.9% to 6.8 ± 0.6%) andadolescents (7.7 ± 0.8% to 7.1 ± 0.6%) (123).
To date, the longest outpatient RCTs lasted 12 weeks and compared HCL treatment (a system that is not currently FDA approved) to sensor-augmented pumps in adults and children as young as 6 years of age (n = 86) with A1C levels above target at baseline. Compared with sensor-augmented pump therapy, the HCL system reduced the risk for hypoglycemia and improved glucose control in A1C levels (124).
Future Systems
A multitude of other automated insulin delivery systems are currently being investigated, including those with dual hormones (insulin and glucagon or insulin and pramlintide). Furthermore, some patients have created do-it-yourself systems through guidance from online communities, although these are not FDA approved or recommended.
6.0.0.0 References
in Emerging Health Technologies. Ottawa, ON, Canadian Agency for Drugs and Technologies in Health, 2016 [Internet]. Available from http:// www.ncbi.nlm.nih.gov/books/NBK476439/. Accessed 22 October 2018