4.4.0.0 Screening and Testing
4.4.1.0 Screening and Testing for Prediabetes and Type 2 Diabetes in Asymptomatic Adults
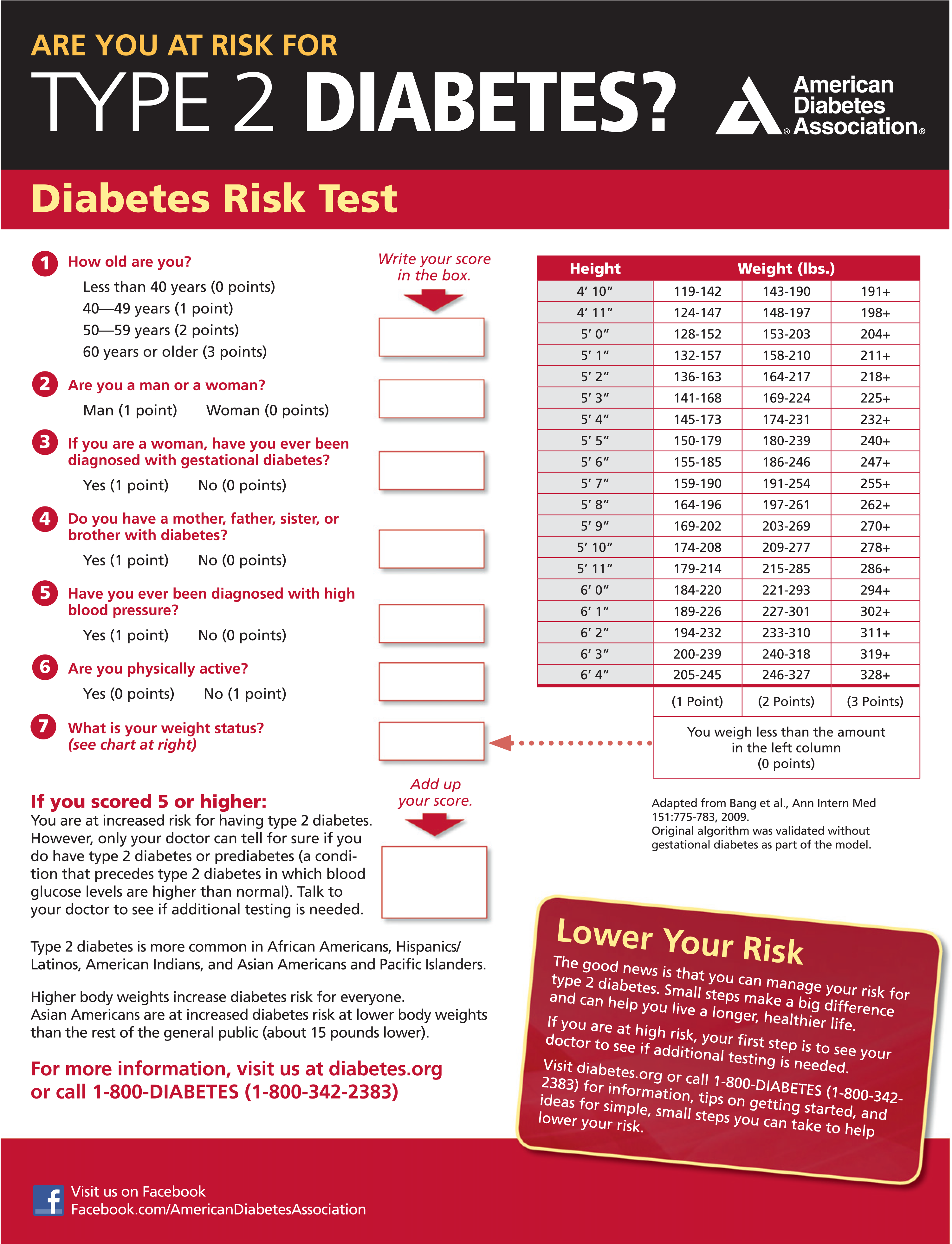
Screening for prediabetes and type 2 diabetes risk through an informal assessment of risk factors (Table 2.3) or with an assessment tool, such as the ADA risk test (Fig. 2.1) (diabetes.org/socrisktest), is recommended to guide providers on whether performing a diagnostic test (Table 2.2) is appropriate. Prediabetes and type 2 diabetes meet criteria for conditions in which early detection is appropriate. Both conditions are common and impose significant clinical and public health burdens. There is often a long presymptomatic phase before the diagnosis of type 2 diabetes. Simple tests to detect preclinical disease are readily available. The duration of glycemic burden is a strong predictor of adverse outcomes. There are effective interventions that prevent progression from prediabetes to diabetes (see Section 3 “Prevention or Delay of Type 2 Diabetes”) and reduce the risk of diabetes complications (see Section 10 “Cardiovascular Disease and Risk Management” and Section 11 “Microvascular Complications and Foot Care”).
Approximately one-quarter of people with diabetes in the U.S. and nearly half of Asian and Hispanic Americans with diabetes are undiagnosed (38,39). Although screening of asymptomatic individuals to identify those with prediabetes or diabetes might seem reasonable, rigorous clinical trials to prove the effectiveness of such screening have not been conducted and are unlikely to occur.
A large European randomized controlled trial compared the impact of screening for diabetes and intensive multifactorial intervention with that of screening and routine care (47). General practice patients between the ages of 40 and 69 years were screened for diabetes and randomly assigned by practice to intensive treatment of multiple risk factors or routine diabetes care. After 5.3 years of follow-up, CVD risk factors were modestly but significantly improved with intensive treatment compared with routine care, but the incidence of first CVD events or mortality was not significantly different between the groups (40). The excellent care provided to patients in the routine care group and the lack of an unscreened control arm limited the authors’ ability to determine whether screening and early treatment improved outcomes compared with no screening and later treatment after clinical diagnoses. Computer simulation modeling studies suggest that major benefits are likely to accrue from the early diagnosis and treatment of hyperglycemia and cardiovascular risk factors in type 2 diabetes (48); moreover, screening, beginning at age 30 or 45 years and independent of risk factors, may be cost-effective (<$11,000 per quality-adjusted life-year gained) (49).
Additional considerations regarding testing for type 2 diabetes and prediabetes in asymptomatic patients include the following.
Figure 2.1 - ADA risk test (diabetes.org/socrisktest).
Age
Age is a major risk factor for diabetes. Testing should begin at no later than age 45 years for all patients. Screening should be considered in overweight or obese adults of any age with one or more risk factors for diabetes.
BMI and Ethnicity
In general, BMI ≥25 kg/m2 is a risk factor for diabetes. However, data suggest that the BMI cut point should be lower for the Asian American population (50,51). The BMI cut points fall consistently between 23 and 24 kg/m2 (sensitivity of 80%) for nearly all Asian American subgroups (with levels slightly lower for Japanese Americans). This makes a rounded cut point of 23 kg/m2 practical. An argument can be made to push the BMI cut point to lower than 23 kg/m2 in favor of increased sensitivity; however, this would lead to an unacceptably low specificity (13.1%). Data from the WHO also suggest that a BMI of ≥23 kg/m2 should be used to define increased risk in Asian Americans (52). The finding that one-third to one half of diabetes in Asian Americans is undiagnosed suggests that testing is not occurring at lower BMI thresholds (53,54).
Evidence also suggests that other populations may benefit from lower BMI cut points. For example, in a large multiethnic cohort study, for an equivalent incidence rate of diabetes, a BMI of 30 kg/m2 in non-Hispanic whites was equivalent to a BMI of 26 kg/m2 in African Americans (55).
Medications
Certain medications, such as glucocorticoids, thiazide diuretics, some HIV medications, and atypical antipsychotics (56), are known to increase the risk of diabetes and should be considered when deciding whether to screen.
Testing Interval
The appropriate interval between screening tests is not known (57). The rationale for the 3-year interval is that with this interval, the number of false-positive tests that require confirmatory testing will be reduced and individuals with false-negative tests will be retested before substantial time elapses and complications develop (57).
Community Screening
Ideally, testing should be carried out within a health care setting because of the need for follow-up and treatment. Community screening outside a health care setting is generally not recommended because people with positive tests may not seek, or have access to, appropriate follow-up testing and care. However, in specific situations where an adequate referral system is established beforehand for positive tests, community screening may be considered. Community testing may also be poorly targeted; i.e., it may fail to reach the groups most at risk and inappropriately test those at very low risk or even those who have already been diagnosed (58).
Screening in Dental Practices
Because periodontal disease is associated with diabetes, the utility of screening in a dental setting and referral to primary care as a means to improve the diagnosis of prediabetes and diabetes has been explored (59-61), with one study estimating that 30% of patients ≥30 years of age seen in general dental practices had dysglycemia (61). Further research is needed to demonstrate the feasibility, effectiveness, and cost-effectiveness of screening in this setting.