xxxxx
1.4.0.0References
- American Diabetes Association. Medical Management of Type 1 Diabetes. 7th ed. Wang CC, Shah AC, Eds. Alexandria, VA, American Diabetes Association, 2017
- American Diabetes Association. Medical Management of Type 2 Diabetes. 7th ed. Burant CF, Young LA, Eds. Alexandria, VA, American Diabetes Association, 2012
- Li R, Zhang P, Barker LE, Chowdhury FM, Zhang X. Cost-effectiveness of interventions to prevent and control diabetes mellitus: a systematic review. Diabetes Care 2010;33:1872– 1894
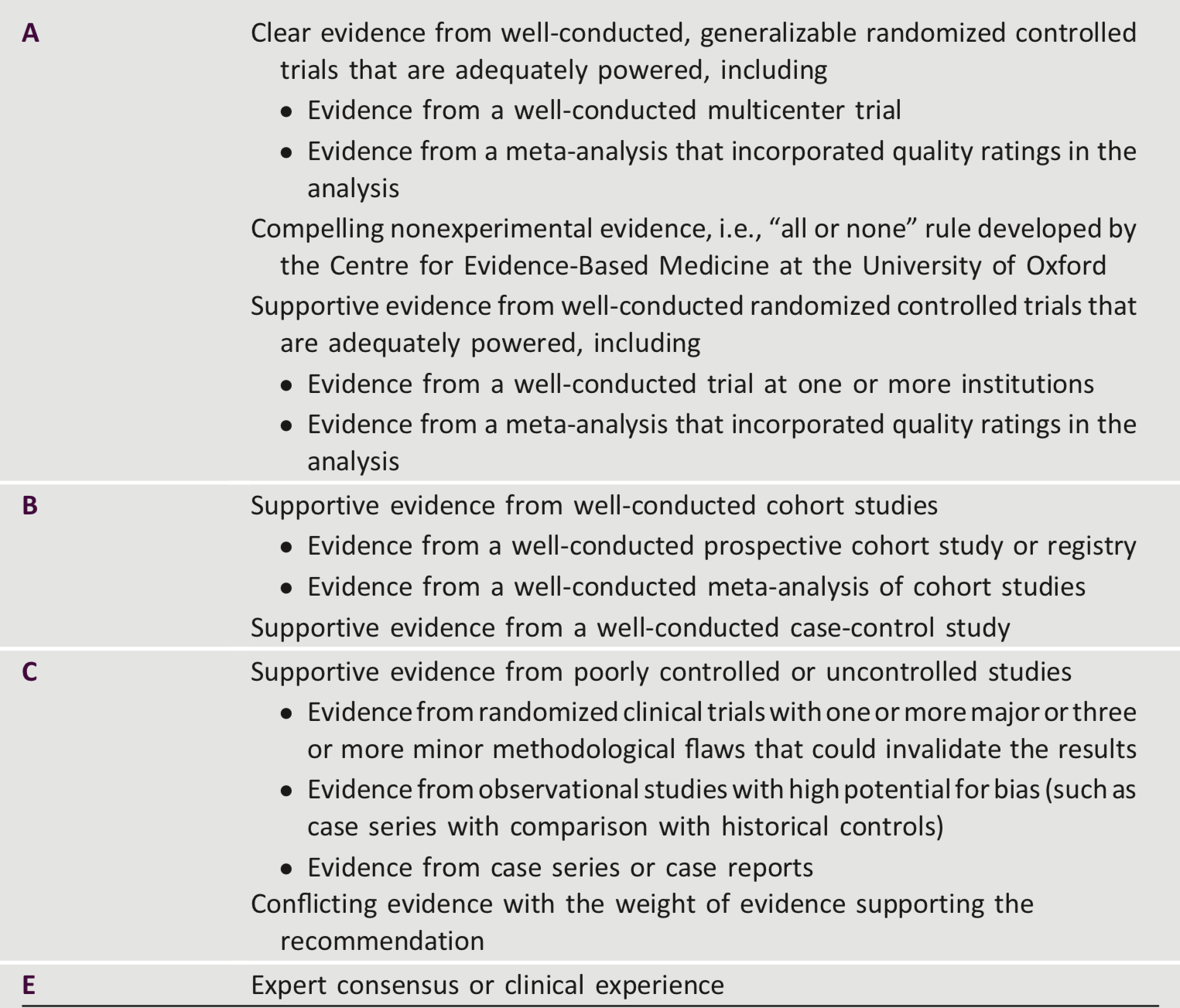
- Grant RW, Kirkman MS. Trends in the evidence level for the American Diabetes Association’s “Standards of Medical Care in Diabetes” from 2005 to 2014. Diabetes Care 2015;38:6–8
xxxxx
2.0.0.0 Professional Practice Committee
The Professional Practice Committee (PPC) of the American Diabetes Association (ADA) is responsible for the “Standards of Medical Care in Diabetes,” referred to as the Standards of Care. The PPC is a multidisciplinary expert committee comprised of physicians, diabetes educators, and others who have expertise in a range of areas, including adult and pediatric endocrinology, epidemiology, public health, lipid research, hypertension, preconception planning, and pregnancy care. Appointment to the PPC is based on excellence in clinical practice and research. Although the primary role of the PPC is to review and update the Standards of Care, it may also be involved in ADA statements, reports, and reviews.
The ADA adheres to the National Academy of Medicine Standards for Developing Trustworthy Clinical Practice Guidelines. All members of the PPC are required to disclose potential conflicts of interest with industry and/or other relevant organizations. These disclosures are discussed at the onset of each Standards of Care revision meeting. Members of the committee, their employers, and their disclosed conflicts of interest are listed in the “Disclosures: Standards of Medical Care in Diabetes – 2019” table (see pp. S184–S186). The ADA funds development of the Standards of Care out of its general revenues and does not use industry support for this purpose.
For the current revision, PPC members systematically searched MEDLINE for human studies related to each section and published since 15 October 2017. Recommendations were revised based on new evidence or, in some cases, to clarify the prior recommendation or match the strength of the wording to the strength of the evidence. A table linking the changes in recommendations to new evidence can be reviewed at professional.diabetes.org/SOC. The Standards of Care was approved by ADA’s Board of Directors, which includes health care professionals, scientists, and lay people. Feedback from the larger clinical community was valuable for the 2018 revision of the Standards of Care. Readers who wish to comment on the 2019 Standards of Care are invited to do so at professional .diabetes.org/SOC.
The PPC would like to thank the following individuals who provided their expertise in reviewing and/or consulting with the committee: Ann Albright, PhD, RD; Pamela Allweiss, MD, MPH; Barbara J. Anderson, PhD; George Bakris, MD; Richard Bergenstal, MD; Stuart Brink, MD; Donald R. Coustan, MD; Ellen D. Davis, MS, RN, CDE, FAADE; Jesse Dinh, PharmD; Steven Edelman, MD; Barry H. Ginsberg, MD, PhD; Irl B. Hirsch, MD; Scott Kahan, MD, MPH; David Klonoff, MD; Joyce Lee, MD, MPH; Randie Little, PhD; Alexandra Migdal, MD; Anne Peters, MD; Amy Rothberg, MD; Jennifer Sherr, MD, PhD; Hood Thabit, MB, BCh, MD, PhD; Stuart Alan Weinzimer, MD; and Neil White, MD.
Members of the PPC
Joshua J. Neumiller, PharmD, CDE, FASCP* (Chair)
Christopher P. Cannon, MD Jill Crandall, MD
David D’Alessio, MD
Ian H. de Boer, MD, MS* Mary de Groot, PhD Judith Fradkin, MD
Kathryn Evans Kreider, DNP, APRN, FNP-BC, BC-ADM
David Maahs, MD, PhD Nisa Maruthur, MD, MHS Medha N. Munshi, MD*
Maria Jose Redondo, MD, PhD, MPH Guillermo E. Umpierrez, MD, CDE, FACE, FACP*
Jennifer Wyckoff, MD
*Subgroup leaders
ADA Nutrition Consensus Report Writing GroupdLiaison
Melinda Maryniuk, MEd, RDN, CDE
American College of CardiologydDesignated Representatives (Section 10)
Sandeep Das, MD, MPH, FACC Mikhail Kosiborod, MD, FACC
ADA Staff
Erika Gebel Berg, PhD (corresponding author: eberg@diabetes.org) Mindy Saraco, MHA
Matthew P. Petersen Sacha Uelmen, RDN, CDE
Shamera Robinson, MPH, RDN William T. Cefalu, MD
xxxxx
3.0.0.0 Summary of Revisions 2019
3.1.0.0 General Changes
The field of diabetes care is rapidly changing as new research, technology, and treatments that can improve the health and well-being of people with diabetes continue to emerge. With annual updates since 1989, the American Diabetes Association (ADA) has long been a leader in producing guidelines that capture the most current state of the field. To that end, the “Standards of Medical Care in Diabetes” (Standards of Care) now includes a dedicated section on Diabetes Technology, which contains preexisting material that was previously in other sections that has been consolidated, as well as new recommendations. Another general change is that each recommendation is now associated with a number (i.e., the second recommendation in Section 7 is now recommendation 7.2). Finally, the order of the prevention section was changed (from Section 5 to Section 3) to follow a more logical progression.
Although levels of evidence for several recommendations have been updated, these changes are not addressed below as the clinical recommendations have remained the same. Changes in evidence level from, for example, E to Care not noted below. The 2019 Standards of Care contains, in addition to many minor changes that clarify recommendations or reflect new evidence, the following more substantive revisions.
xxxxx
3.2.0.0.Section Changes
3.2.1.0 Section 1
Additional information was included on the financial costs of diabetes to individuals and society.
Because telemedicine is a growing field that may increase access to care forpatients withdiabetes, discussion was added on its use to facilitate remote delivery of health-related services and clinical information.
xxxxx
3.2.2.0 Section 2
Based on new data, the criteria for the
diagnosis of diabetes was changed to include two abnormal test results from the same sample (i.e., fasting plasma glucose and A1C from same sample). The section was reorganized to improve flow and reduce redundancy. Additional conditions were identified that may affect A1C test accuracy including the postpartum period.
xxxxx
3.2.3.0 Section 3
This section was moved (previously it was Section 5) and is now located before the Lifestyle Management section to better reflect the progression of type 2 diabetes. The nutrition section was updated to highlight the importance of weight loss for those at high risk for developing type 2 diabetes who have overweight or obesity.
Because smoking may increase the risk of type 2 diabetes, a section on tobacco use and cessation was added.
xxxxx
3.2.4.0 Section 4
On the basis of a new consensus report on diabetes and language, new text was added to guide health care professionals’ use of language to communicate about diabetes with people with diabetes and professional audiences in an informative, empowering, and educational style.
A new figure from the ADA-European Association for the Study of Diabetes(EASD) consensus report about the diabetes care decision cycle was added to emphasize the need for ongoing assessment and shared decision making to achieve the goals of health care and avoid clinical inertia.
A new recommendation was added to explicitly call out the importance of the diabetes care team and to list the professionals that make up the team.
The table listing the components of a comprehensive medical evaluation was revised, and the section on assessment and planning was used to create a new table (Table 4.2).
A new table was added listing factors that increase risk of treatment-associated hypoglycemia (Table 4.3).
A recommendation was added to include the 10-year atherosclerotic cardiovascular disease (ASCVD) risk as part of overall risk assessment.
The fatty liver disease section was revised to include updated text and a new recommendation regarding when to test for liver disease.
xxxxx
3.2.5.0 Section 5
Evidence continues to suggest that there is not an ideal percentage of calories from carbohydrate, protein, and fat for all people with diabetes. Therefore, more discussion was added about the importance of macronutrient distribution based on an individualized assessment of current eating patterns, preferences, and metabolic goals. Additional considerations were added to the eating patterns, macronutrient distribution, and meal planning sections to better identify candidates for meal plans, specifically for low-carbohydrate eating patterns and people who are pregnant or lactating, who have or are at risk for disordered eating, who have renal disease, and who are taking sodium–glucose cotransporter 2 inhibitors. There is not a one-size-fits-all eating pattern for individuals with diabetes, and meal planning should be individualized.
A recommendation was modified to encourage people with diabetes to decrease consumption of both sugar sweetened and nonnutritive-sweetened beverages and use other alternatives, with an emphasis on water intake.
The sodium consumption recommendation was modified to eliminate the further restriction that was potentially indicated for those with both diabetes and hypertension.
Additional discussion was added to the physical activity section to include the benefit of a variety of leisure-time physical activities and flexibility and balance exercises. The discussion about e-cigarettes was expanded to include more on public perception and how their use to aide smoking cessation was not more effec-
tive than “usual care.”
xxxxx
3.2.6.0 Section 6
This section now begins with a discussion of A1C tests to highlight the centrality of A1C testing in glycemic management. The self-monitoring of blood glucose and continuous glucose monitoring text and recommendations were moved to the new Diabetes Technology section.To emphasize that the risks and benefits of glycemic targets can change as diabetes progresses and patients age, a recommendation was added to reevaluate glycemic targets over time.
The section was modified to align with the living Standards updates made in April 2018 regarding the consensus definition of hypoglycemia.
xxxxx
3.2.7.0 Section 7
This new section includes new recommendations, the self-monitoring of blood glucose section formerly included in Section 6 “Glycemic Targets,” and a discussion of insulin delivery devices (syringes, pens, and insulin pumps), blood glucose meters, continuous glucose monitors (real-time and intermittently scanned [“flash”]), and automated insulin delivery devices.
The recommendation to use selfmonitoring of blood glucose in people who are not using insulin was changed to acknowledge that routine glucose monitoring is of limited additional clinical benefit in this population.
xxxxx
3.2.8.0 Section 8
A recommendation was modified to
acknowledge the benefits of tracking weight, activity, etc., in the context of achieving and maintaining a healthy weight.
A brief section was added on medical devices for weight loss, which are not currently recommended due to limited data in people with diabetes.
The recommendations for metabolic surgery were modified to align with recent guidelines, citing the importance of considering comorbidities beyond diabetes when contemplating the appropriateness of metabolic surgery for a given patient.
xxxxx
3.2.9.0 Section 9
The section on the pharmacologic treatment of type 2 diabetes was significantly changed to align, as per the living Standards update in October 2018, with the ADA-EASD consensus report on this topic, summarized in the new Figs. 9.1 and 9.2. This includes consideration of key patient factors:
a) important comorbidities such as ASCVD, chronic kidney disease, and heart failure, b) hypoglycemia risk, c) effects on body weight, d side effects, e) costs, and f) patient preferences. To align with the ADA-EASD consensus report, the approach to injectable medication therapy was revised (Fig. 9.2). A recommendation that, for most patients who need the greater efficacy of an injectable medication, a glucagon-like peptide 1 receptor agonist should be the first choice, ahead of insulin.
A new section was added on insulin injection technique, emphasizing the importance of technique for appropriate insulin dosing and the avoidance of complications (lipodystrophy, etc.).
The section on noninsulin pharmacologic treatments for type 1 diabetes was abbreviated, as these are not generally recommended.
xxxxx
3.2.10.0 Section 10
For the first time, this section is endorsed
by the American College of Cardiology. Additional text was added to acknowledge heart failure as an important type of cardiovascular disease in people with diabetes for consideration when determining optimal diabetes care.
The blood pressure recommendations were modified to emphasize the importance of individualization of targets based on cardiovascular risk.
A discussion of the appropriate use of the ASCVD risk calculator was included, and recommendations were modified to include assessment of 10-year ASCVD risk as part of overall risk assessment and in determining optimal treatment approaches.
The recommendation and text regarding the use of aspirin in primary prevention was updated with new data.
For alignment with the ADA-EASDconsensus report, two recommendations were added for the use of medications thathave proven cardiovascular benefit in people with ASCVD, with and without heart failure.
xxxxx
3.2.11.0 Section 11
To align with the ADA-EASD consensus
report, a recommendation was added for people with type 2 diabetes and chronic kidney disease to consider agents with proven benefit with regard to renal outcomes.
The recommendation on the use of telemedicine in retinal screening was modified to acknowledge the utility of this approach, so long as appropriate referrals are made for a comprehensive eye examination.
Gabapentin was added to the list of agents to be considered for the treatment of neuropathic pain in people with diabetes based on data on efficacy and the potential for cost savings.
The gastroparesis section includes a discussion of a few additional treatment modalities.
The recommendation for patients with diabetes to have their feet inspected at every visit was modified to only include those at high risk for ulceration. Annual examinations remain recommended for everyone.
xxxxx
3.2.12.0 Section 12
A new section and recommendation on lifestyle management was added to address the unique nutritional and physical activity needs and considerations for older adults. Within the pharmacologic therapy discussion, deintensification of insulin regimes was introduced to help simplify insulin regimen to match individual’s self-management abilities. A new figure was added (Fig. 12.1) that provides a path for simplification. A new table was also added (Table 12.2) to help guide providers considering medication regimen simplification and deintensification/deprescribing in older adults with diabetes.
xxxxx
3.2.13.0 Section 13
Introductory language was added to the beginning of this section reminding the reader that the epidemiology, pathophysiology, developmental considerations, and response to therapy in pediatric-onset diabetes are different from adult diabetes, and that there are also differences in recommended care for children and adolescents with type 1 as opposed to type 2 diabetes.
A recommendation was added to emphasize the need for disordered eating screening in youth with type 1 diabetes beginning at 10–12 years of age.
Based on new evidence, a recommendation was added discouraging e-cigarette use in youth.
The discussion of type 2 diabetes in children and adolescents was significantly expanded, with new recommendations in a number of areas, including screening and diagnosis, lifestyle management, pharmacologic management, and transition of care to adult providers. New sections and/or recommendations for type 2 diabetes in children and adolescents were added for glycemic targets, metabolic surgery, nephropathy, neuropathy, retinopathy, nonalcoholic fatty liver disease, obstructive sleep apnea, polycystic ovary syndrome, cardiovascular disease, dyslipidemia, cardiac function testing, and psychosocial factors. Figure 13.1 was added to provide guidance on the management of diabetes in overweight youth.
xxxxx
3.2.14.0 Section 14
Women with preexisting diabetes are now recommended to have their care managed in a multidisciplinary clinic to improve diabetes and pregnancy outcomes.
Greater emphasis has been placed on the use of insulin as the preferred medication for treating hyperglycemia in gestational diabetes mellitus as it does not cross the placenta to a measurable extent and how metformin and glyburide should not be used as firstline agents as both cross the placenta to the fetus.
xxxxx
3.2.15.0 Section 15
Because of their ability to improve hospital readmission rates and cost of care, a new recommendation was added calling for providers to consider consulting with a specialized diabetes or glucose management team where possible when caring for hospitalized patients with diabetes.
xxxxx
3.2.16.0 Section 16
The “Insulin Access and Affordability Working Group: Conclusions andRecommendations” ADA statement was added to this section. Published in 2018, this statement compiled public information and convened a series of meetings with stakeholders throughout the insulin supply chain to learn how each entity affects the cost of insulin for the consumer, an important topic for the ADA and people living with diabetes.